
Thoracic Surgery General Management IV Complications
Author: Brian Mitzman, MD
Institution: University of Utah
Date Reviewed: March 2025
Learning Domain: General Thoracic
Learning Objective: Diagnosis and treatment of common complications
PowerPoint File: ![]() TS04 - Post-lobectomy Complications.pptx
TS04 - Post-lobectomy Complications.pptx
Learning Goals
- The basic level concepts focused on:
- General Knowledge
- Diagnosis and Treatment of common complications
Discussion Questions
- Most common complications after lobectomy?
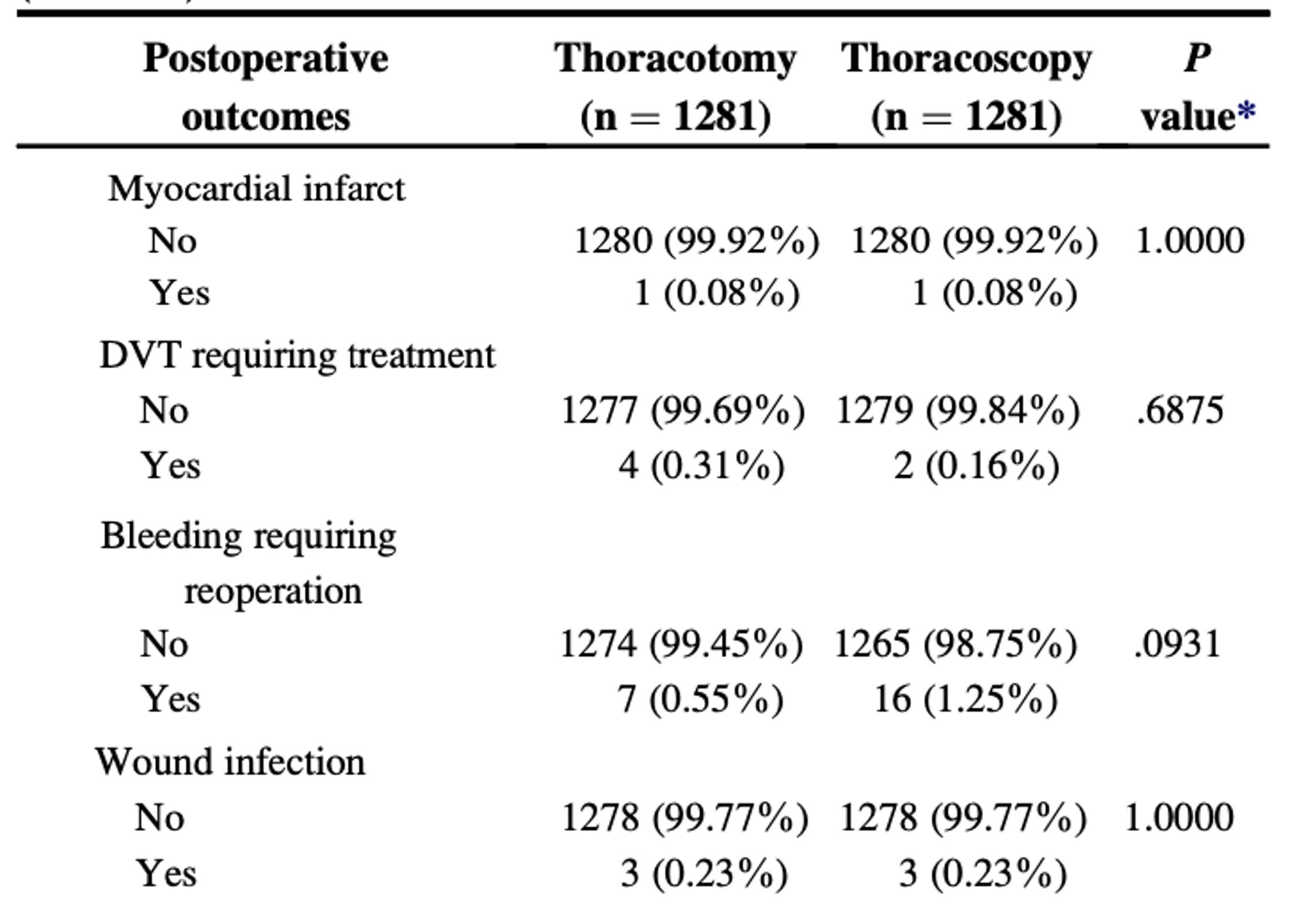
Historical Data from STS Database
From: Subroto P, et al. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: a Propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg 2010;139:366-78

Less common complications:
Data from STS GTSD 2022 Summary
From: Servais et al. Ann Thorac Surg. 2023;115:43-50
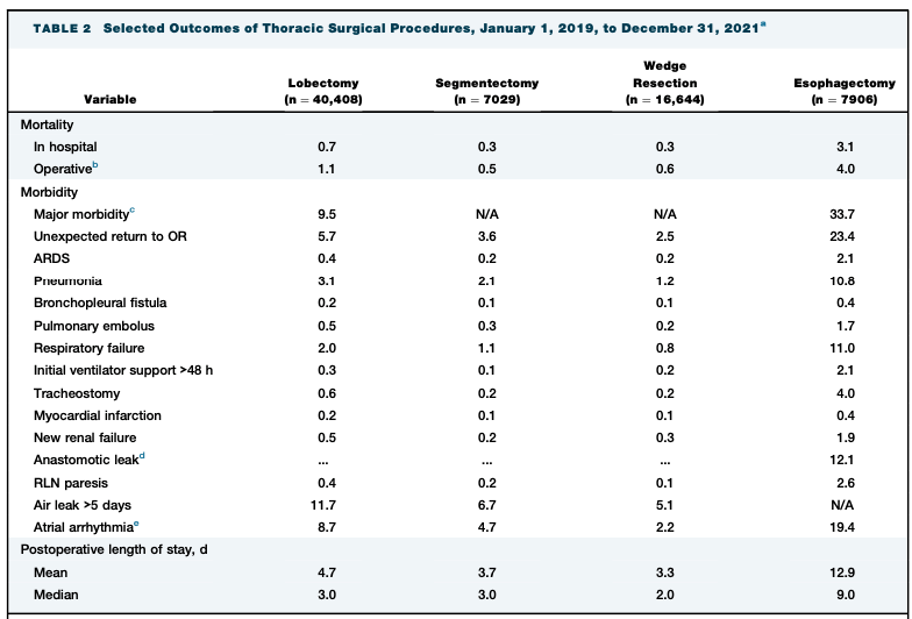
Lobectomy
- Overall Major Morbidity: 9.5%
- Atrial Arrhythmia: 8.7%
- Pneumonia: 3.1%
- MI: 0.2%
- Length of Stay: Median 3.0 Days
Prolonged Air Leak (>5 Days)
- Lobectomy: 11.7%
- Segmentectomy: 6.7%
- Wedge: 5.1%
Case #1
- 74 y/o M with COPD (baseline FEV1 54%, DLCO 55%) undergoes uncomplicated robotic right upper lobectomy.
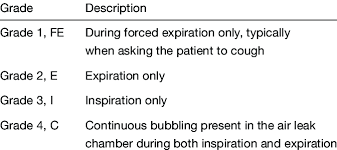
- POD #1: Single chest tube to -20 suction. Air leak is E2-3 (expiratory bubbling into 2-3 chambers). CXR no pneumothorax.
- What do you do, if anything?
Discussion
Topic for discussion:
- Stay on suction versus waterseal?
- Decrease suction from -20 to -10?
- Intervene now? If so, how?
- Observation? For how long?
Case #1
- You opt to observe.
- It is now POD #5. Chest tube has been watersealed without pneumothorax, but air leak remains E1.
- What now?
Treatment
- Discharge home with portable device and give more time
Other Options
Autologous Blood Patch
- 50-100cc of peripheral venous blood injected through chest tube
- Tube/pleurevac then elevated to allow air to escape but blood to remain
- Success rate reported 50-90%
- Risk of empyema (0-9%)
Chemical Pleurodesis
- Talc, doxycycline, iodine, other
Endobronchial Valve
Case #2
- 71 y/o M undergoes robotic left lower lobectomy for a Stage Ib adenocarcinoma. The patient has no major cardiac history. His wife read that atrial fibrillation is a common complication and wants to know if she should worry.
- What do you tell her?
Discussion
- What are the risk factors for postoperative atrial fibrillation?
- Is there a role for prophylactic medical treatment after lung surgery?
- How do you treat acute onset a-fib in the postoperative lobectomy patient?
Prophylaxis
Class I
- Patients taking B-blockers preoperatively should continue treatment postoperatively (level B)
Class IIa
- Cardizem prophylaxis is reasonable if not taking BB (level B)
- Amiodorone prophylaxis is reasonable (level B)
- Magnesium supplementation is reasonable to augment effects of other medications (level B)
Class IIb
- New initiation of BB postoperatively for prophylaxis may be reasonable, but use is more limited by side effects than Cardizem (level B)
Class III
- Amiodorone not recommended for pneumonectomy patients due to toxicity (level B)
- Digitalis should not be used for prophylaxis (Level A)
- Flecainide is not recommended for prophylaxis (Level B)
Fernando HC et al. The Society of Thoracic Surgeons practice guideline on the prophylaxis and management of atrial fibrillation associated with general thoracic surgery: executive summary. Ann Thorac Surg. 2011 Sep;92(3):1144-52. doi: 10.1016/j.athoracsur.2011.06.104. PMID: 21871327.
Acute Treatment of Postoperative A-Fib
Class I
- Electrical cardioversion for patients who are hemodynamically unstable (level C)
- Hemodynamically stable but symptomatic should be chemically cardioverted. Electrical cardioversion if chemical fails (Level C)
- Hemodynamically stable with symptomatically acceptable AF should have trial of rate control lasting 24 hours (Level B)
Class IIa
If hemodynamically stable and lasting 24 hours or longer after rate control, reasonable to attempt chemical cardioversion (Level C)
Class IIb
Hemodynamically stable AF refractory to chemical cardioversion should be considered for electrical cardioversion (Level C)
Fernando HC et al. The Society of Thoracic Surgeons practice guideline on the prophylaxis and management of atrial fibrillation associated with general thoracic surgery: executive summary. Ann Thorac Surg. 2011 Sep;92(3):1144-52. doi: 10.1016/j.athoracsur.2011.06.104. PMID: 21871327.
Choice of Agent for Rate Control
Class I
- Selective B1 blocking agent recommended for initial rate control in absence of moderate-severe COPD or bronchospasm (level B)
- Diltiazem should be first line agent in presence of COPD or bronchospasm (Level B)
Class III
- Digoxin as a single agent should not be used for rate control, but may be effective as combination with B1 or diltiazem (level A)
Fernando HC et al. The Society of Thoracic Surgeons practice guideline on the prophylaxis and management of atrial fibrillation associated with general thoracic surgery: executive summary. Ann Thorac Surg. 2011 Sep;92(3):1144-52. doi: 10.1016/j.athoracsur.2011.06.104. PMID: 21871327.
Learning Points
- Atelectasis, atrial arrhythmia, air leak, pneumonia are common complications after lobectomy, even in modern era.
- Most air leaks stop spontaneously, and a trial at home with portable chest tube device is reasonable. Numerous methods for intervention are available if unsuccessful.
- Atrial fibrillation prophylaxis is not universally accepted, however, guidelines exist to help provide direction.