Thoracic Surgery General Management III
Author: Ammar Asban, MD & Brian Mitzman, MD
Institution: University of Utah
Date Reviewed: March 2025
Original Case: Stephen Yang, MD
Learning Domain: General Thoracic
Learning Objective: Risk assessment and postoperative complications for pneumonectomy
PowerPoint File: ![]() TS03 - Thoracic Surgery General Management III.pptx
TS03 - Thoracic Surgery General Management III.pptx
Learning Goals
- The basic level concepts focused on:
- Risk Assessment: Lung
- The advanced level concepts focused on:
- Postop Complications: Lung
Case #1
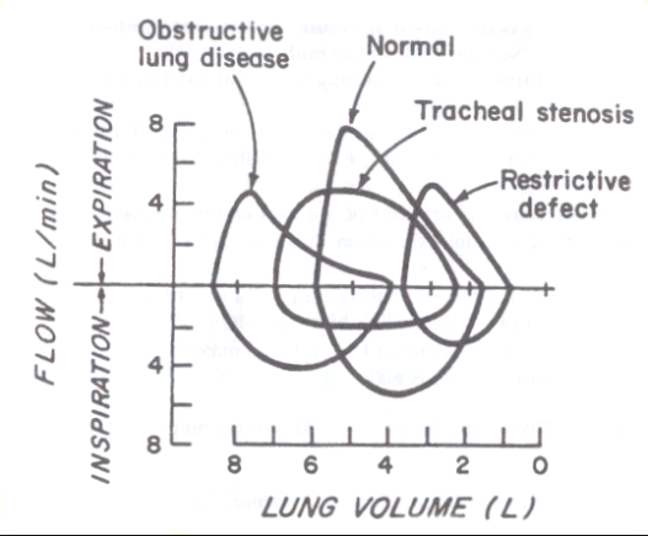
60 yo M presents with SOB on exertion. PFTs are performed. What does this P/V flow loop show?
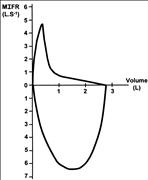
Discussion
Case #2 Part 1
- 68 yo F presents for evaluation of a localized 2 cm NSCLC of the lingula.
- Work up included:
- ppoFEV1 30%
- DLCO 40%
- ECHO LVEF 50%, RVSP 30
- MVO2 max 8 ml/kg/min
- What should we offer this patient surgically, if anything?
Case #2 Part 2
- 68 yo F undergoes a RML/RLL bilobectomy.
- You reinflate the remaining RUL, but worry there will be a significant pleural space left.
- What are some maneuvers to minimize the pleural space?
Case #2 Part 3
1 after RLL lobectomy for NSCLC, you look at the patient and see this? What is going on and what do you do?

Case #3
- A 72 yo undergoes a VATS RUL lobectomy with lymph node dissection having a positive R10 LN
- On POD3, she is eating and walking with one chest tube
- The chest tube drainage begins to increase to between 1000-1500 cc of opalescent fluid in 24 hours.
- No organisms are identified in the fluid
- Diagnosis?
- Initial management should include?
Management of Chylothorax
- In postoperative setting
- Dietary control measures, fasting, low-fat diet and total parenteral nutrition
- What will you do if there is evidence of mediastinal shift?
- Adjunct therapy
- Somatostatin, octreotide, and midodrine
- How long would you monitor this patient and what type of intervention would you consider?
- Pleurodesis
- Thoracic duct embolization
- Thoracic duct disruption
- Thoracic duct ligation
- Combination therapy

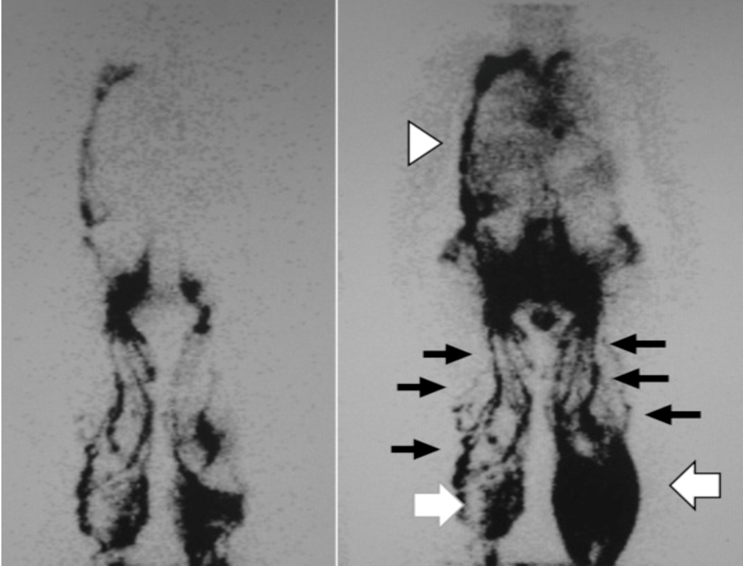
Therapeutic lymphangiography for traumatic chylothorax. Hara et al. Journal of Vascular Surgery: Venous and Lymphatic Disorders, Volume 6, Issue 2, March 2018, Pages 237-240
Case #4
- 60 yo M construction worker with a 40-pack year smoking history was evaluated for resection of a carcinoma involving the bronchus intermedius
- Preoperative pulmonary function tests showed FVC = 2.5L, FEV1 = 1.8 L, DLCO = 35% of predicted, room air Pa02 = 60 mmHg
- What do his PFTs suggest and should he undergo resection?
Case #5 Part 1
- A 55 yo underwent a difficult right pneumonectomy for advanced NSCLC requiring intrapericardial dissection vessel control.
- Preop PFTs were excellent and he is generally healthy
- POD2 he develops sudden SVT, hypotension and desaturation.
- Initial management of his SVT is unsuccessful
- CXR is shown. What next?

Case #5 Part 2
- 3 days after right pneumonectomy patient noted to have a new LLL infiltration, cough, frothy sputum, and respiratory failure
- What is your differential diagnosis?
- How will you proceed to work this up?
- What is the most common cause?
- How would you manage this patient?
- What operation would you offer this patient?
Case #5 Part 3
- 6 weeks after right pneumonectomy patient comes to clinic with fever, new onset cough productive blood-tinged sputum. CXR shows air-fluid level in the right hemothorax
- What is your work up?
- What your differential diagnosis?
- How would you manage this patient?
Case #6
- Your 71yo M patient is undergoing a routine RUL VATS lobectomy.
- Prior to induction of anesthesia, a right subclavian catheter is placed for IV access.
- During placement develops pulmonary wheezing, tachypnea, and tachycardia. Physical exam reveals a "mill wheel" churning murmur.
- What is done next?
Case #7
- A 72 yo M is 1 year out following R pneumonectomy for T2N0 NSCLC Has been doing well except for progressive SOB since surgery Particularly worse since the last clinic visit 4 months ago
- CXR is shown
- What next?
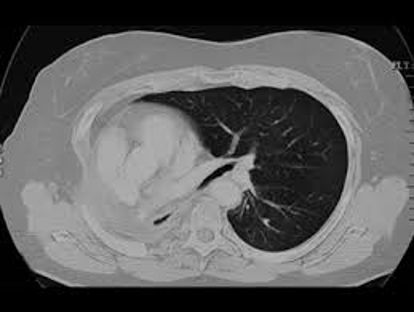
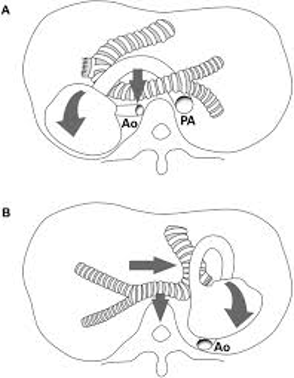
Discussion: Post-pneumonectomy Syndrome

Case #8
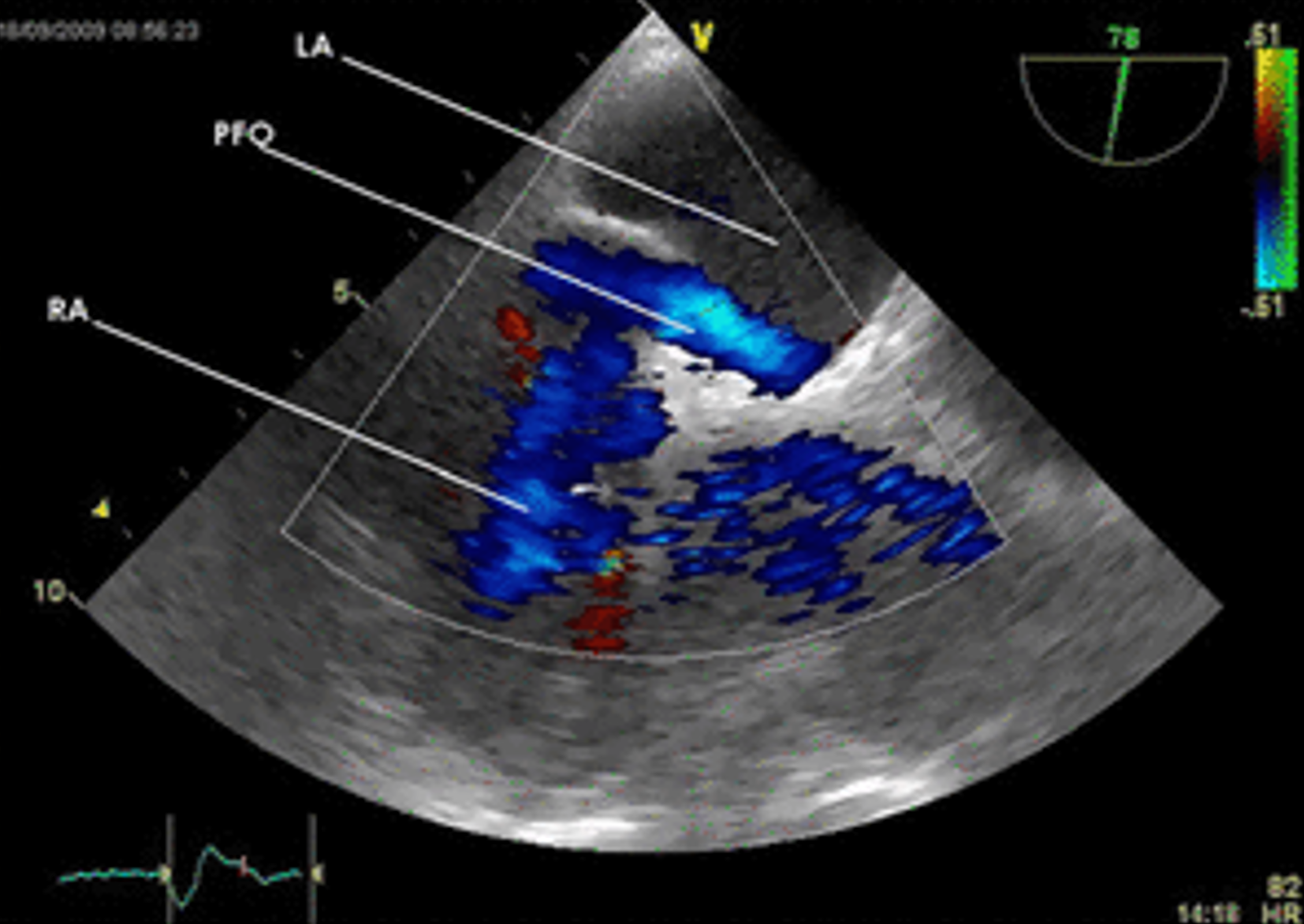
- 65-year-old man underwent uneventful right pneumonectomy for lung cancer.
- POD1, he experienced profound dyspnea when standing. His BP was 120/80 with a HR of 88 both standing and supine. His O2 sat was 92% on room air while in the supine position and was 80% in the standing position.
- The patient has no significant cardiopulmonary history and his preoperative pulmonary function tests were excellent.
- What is done next? What is the diagnosis?
Discussion: Platypnea-orthodeoxia