Neoplasms of the Lung II
Author: Paul Schipper, MD
Institution: OHSU
Date Reviewed: March 2025
Original Case: Stephen C. Yang, MD
Learning Domain: General Thoracic
Learning Objective: Stage I Staging, including all staging tools, Stage I survival and recurrence patterns. Advanced level concepts focus on Stage I treatment and Multimodality
PowerPoint File: ![]() Neoplasms of the Lung II.pptx
Neoplasms of the Lung II.pptx
History
- 64-yo was found to have an apical RUL lung nodule on a screening CXR
- Patient has no pulmonary symptoms
- Former 30 py smoker, quit 10 years ago
- PMH: hypertension, arthritis
- No prior surgeries
- ECOG PS0
Physical Exam
- Gen: WNWD NAD, appears stated age
- CV: RRR no m,g,r
- CHEST: BS equal and clear
- ABD: soft, flat non tender
- EXT: no edema
Work Up
- Labs WNL
- Coags WNL
- PFTs
- FEV-1 = 1.84 L (87% predicted)
- FVC = 2.21 (81% predicted)
- DLCO = 14.5 (68% predicted)
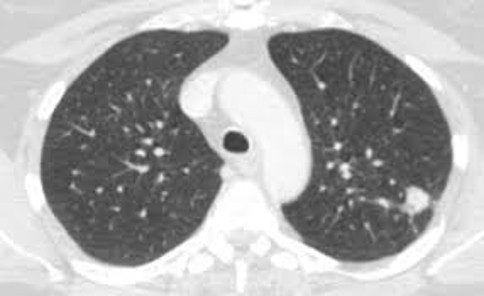
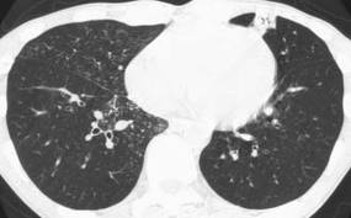
CT Scan
3 cm mass apex of RUL. No hilar or mediastinal adenopathy. Upper cuts of abdomen normal.
Differential Diagnosis?
- Neoplasm
- Infection
- Congenital
- Trauma
- Other
- Next steps?
PET/CT Scan
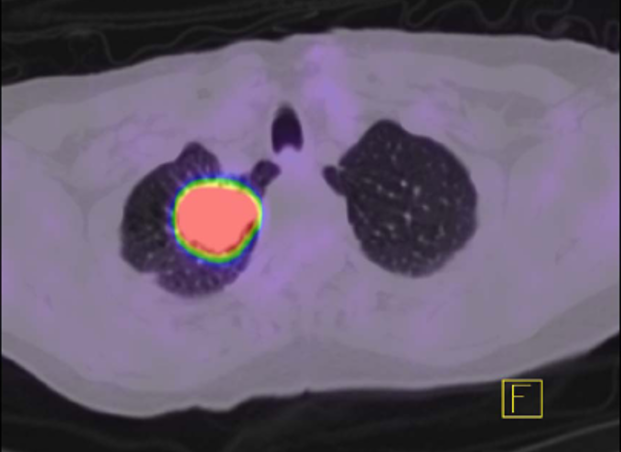
Integrated scan showing hypermetabolic activity only in the lung mass. No uptake elsewhere.
Outcome
- Underwent VATS RUL lobectomy
- Uncomplicated postoperative course
- Final path shows a 3.3 cm adenocarcinoma, lymph nodes in 4R, 7, 9R, and 10 R negative (3+1)
- What stage is this?
- Adjuvant therapy?
- Surveillance?
- 5 year survival?
3.3 cm = T2a
T2aN0M0 = Stage IB
No adjuvant therapy offered other than clinical trial
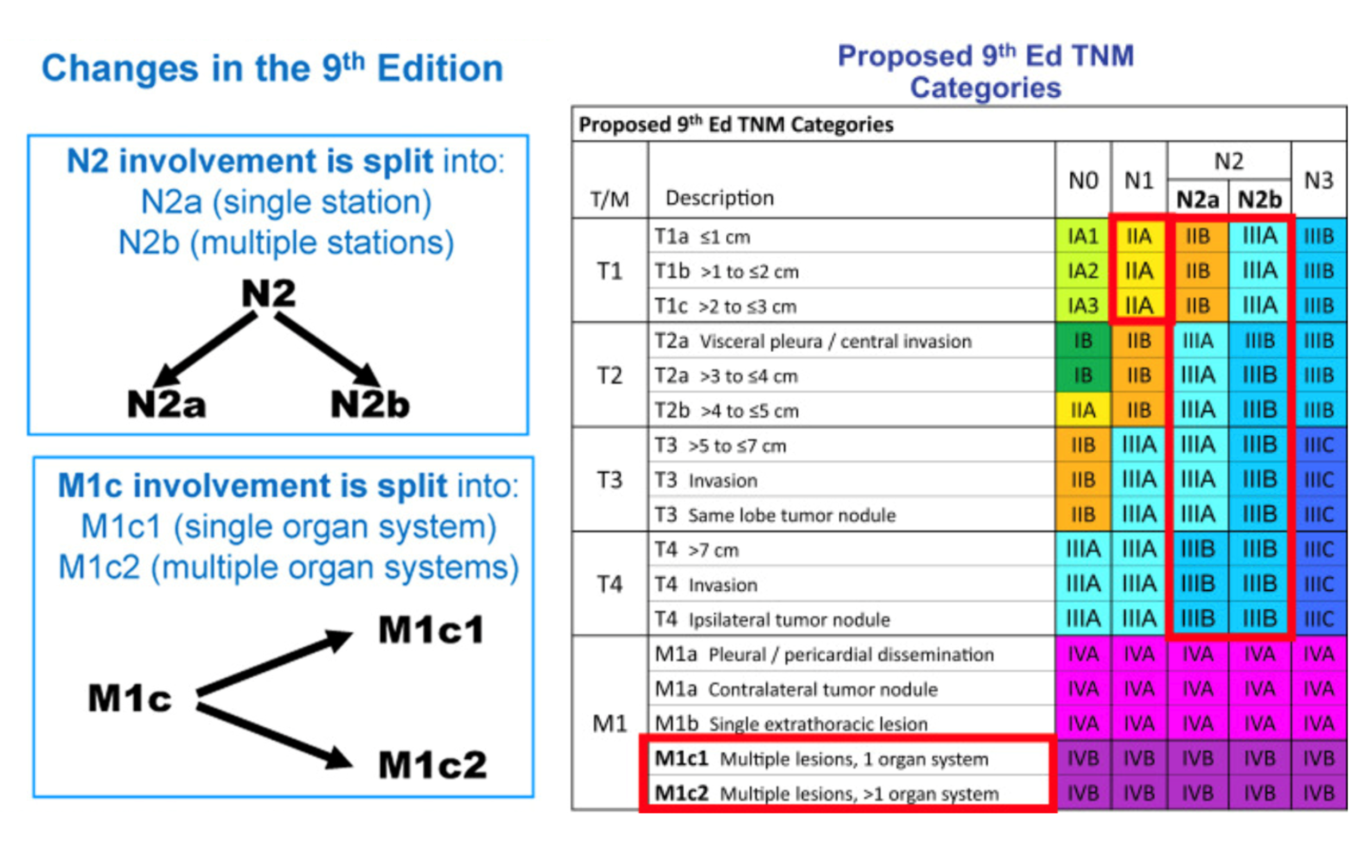
Journal of Thoracic Oncology, Volume 19, Issue 7, July 2024, Pages 1007-1027.
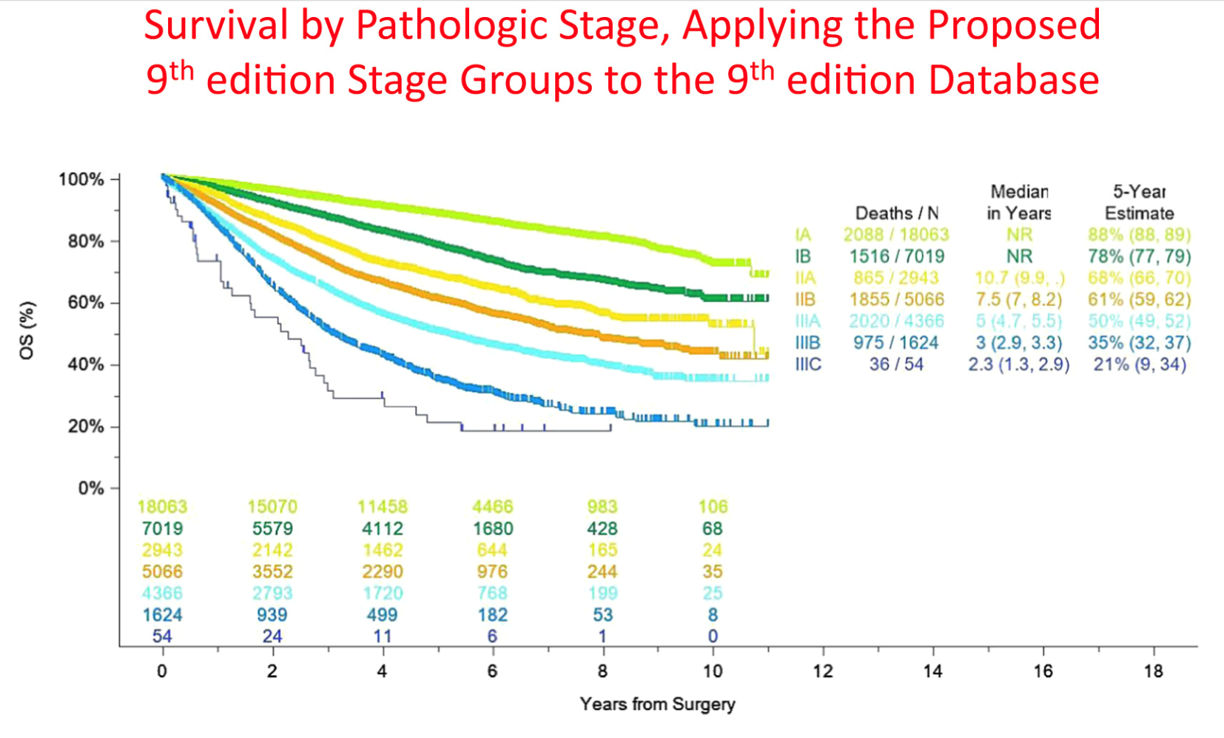
Journal of Thoracic Oncology, Volume 19, Issue 7, July 2024, Pages 1007-1027.
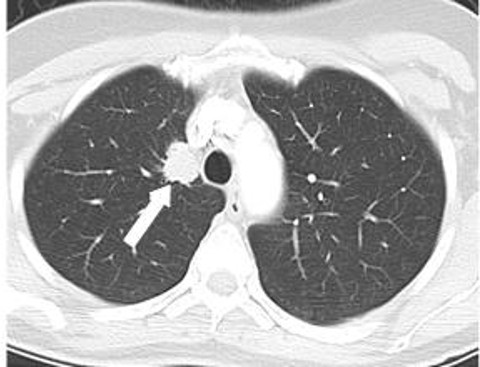
History
- A 78 year-old M presents with a 2cm spiculated mass in the lingular tip found on w/u for dry cough
- Former 30 py smoker, quit 20 years ago
- PMH: rheumatoid arthritis, HTN, DM
- No prior surgeries
- ECOG PS0
Work Up
- PE: Normal
- Labs WNL
- CXR and CT confirm the same 2 cm mass in the lingular tip.
- There is a 1.5 cm AP window node, no other hilar or mediastinal adenopathy
- PFTs:
- FEV-1 = 1.7 L (65% predicted)
- FVC = 2.1 (71% predicted)
- DLCO = 20.5 (88% predicted)
- Next steps?
Discussion Points
- Role of PET scanning? EBUS? Mediastinoscopy? Chamberlain Procedure? Needle aspiration?
- Role of mediastinal lymph node dissection?
- Lung sparing options?
- What if left upper lobe rather than just lingula?
- What if lymph node positive on mediastinoscopy?
- After final path report?
Outcome
- PET showed avidity in the lung nodule only
- EBUS stations L4, 7, and L10 negative
- Mediastinoscopy negative
- Left VATS lingulectomy, mediastinal LN dissection
- What if AP window was positive intraop?
- Final path T1N0 adenocarcinoma
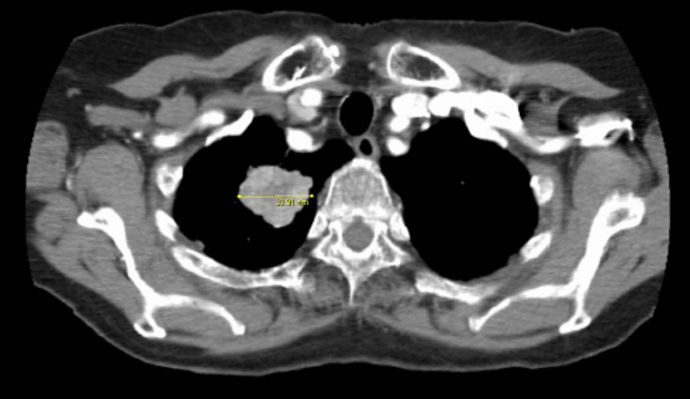
History
- A 75 yo M is referred for a PET positive lung mass found on w/u for SOB
- Former heavy smoker
- PMH: CAD, PVD, HTN
- No prior surgeries
- ECOG PS0
- PFTs:
- FEV1 40% predicted,
- DLCO 45% predicted
- ECHO: LVEF 55%,
- PAS est 40 mmHg, mild TR
- PET: avidity only in lung mass
- What are options?