
Undifferentiated Pleomorphic Sarcoma of the Chest Wall
Author: Paul Schipper, MD
Institution: OHSU
Date Reviewed: March 2025
Original Case: Dale Han, MD
Learning Domain: General Thoracic
Learning Objective: Diagnosis and management of undifferentiated pleomorphic sarcoma
PowerPoint File: ![]() Undifferentiated Pleomorphic Sarcoma of the Chest Wall.pptx
Undifferentiated Pleomorphic Sarcoma of the Chest Wall.pptx
History
- 72 year-old female with history of right breast cancer treated with lumpectomy and radiation. Eight years later, she develops a right anterolateral chest wall mass
- PMH:
- Right breast cancer, hypertension, pancreatitis
- PSH:
- Right breast lumpectomy, hysterectomy, umbilical hernia repair, bilateral tubal ligation
- SH:
- 10 pack year smoking history. Quit 45 years ago
Exam and Labs
Pertinent Physical Exam
- Lungs clear bilaterally
- Heart rate regular
- Right chest in lower right axilla with an approximately 5 cm hard fixed mass, no skin changes
Labs
- Normal white cell count
Chest CT
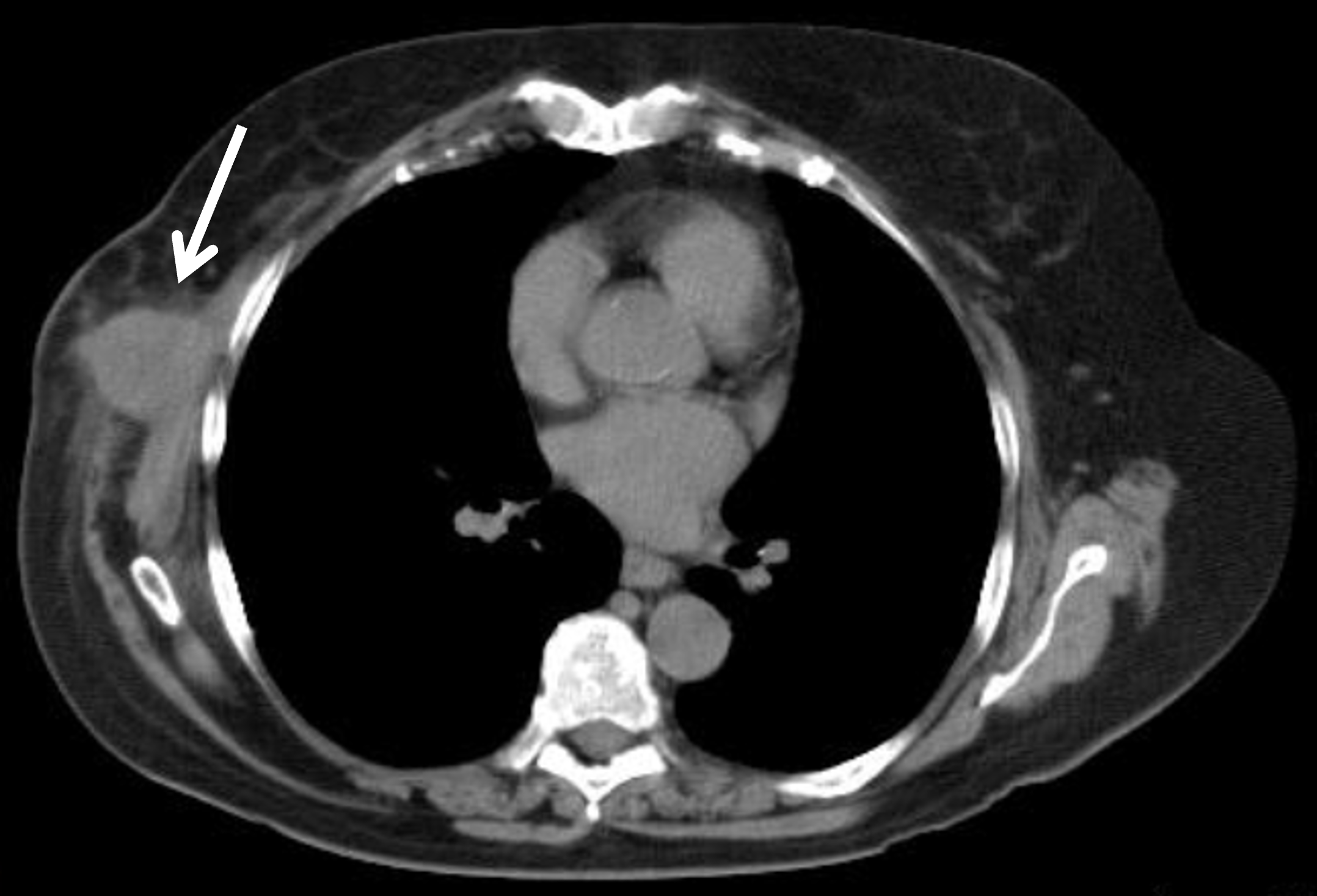
CT chest: 4.6 cm lobulated mass in right axilla next to 6th and 7th ribs, no pulmonary nodules
Additional Studies
- Brain MRI
- PET scan
Discussion Points for Conference
- Differential Diagnosis?
- Diagnostic Approaches ?
- Core Needle Biopsy
- Incisional Biopsy
- Excisional Biopsy
- Therapeutic Options ?
- Radiation Therapy
- Wide excision
- Combined modalities
- Stage?
Further Work Up
- Core needle biopsy of mass: atypical spindle cells
- Excisional biopsy performed resecting mass down to and including portion of serratus anterior muscle
- Pathology: undifferentiated pleomorphic sarcoma
- 4.2 cm
- Grade 2
- Positive deep and caudal margins
- MRI brain: negative for metastases
- PET scan: negative for metastases
Surgery
- Patient subsequently referred and evaluated for definitive management of right chest wall sarcoma
- Right chest radical resection of excisional biopsy cavity with en bloc resection of right ribs 4, 5, 6, 7
- Wedge resections of 2 right lower lobe pulmonary nodules found intra-operatively
- Reconstruction of chest wall with mesh and latissimus dorsi flap

Pathology: Residual cells with morphologic appearance similar to original sarcoma. Margins negative. Pulmonary wedge resections negative for malignancy.
Further Discussion Points
- Development of sarcoma in radiated tissue
- Use of excisional biopsy versus upfront radical resection of chest wall
- Extent of resection: en-bloc resection of ribs for positive deep margin after resection of serratus anterior muscle
- Reconstruction of defect
- Adjuvant therapy for chest wall sarcomas
Learning Points
- Undifferentiated pleomorphic sarcoma previously known as malignant fibrous histiocytoma
- Attempt needle biopsy as opposed to excisional biopsy to minimize extent of final resection
- Atypical spindle cells on needle biopsy should be assumed to be sarcoma in the appropriate clinical setting
- Radical wide excision is treatment with resection of involved structures such as ribs and chest wall
- Local recurrence common (20-45%)
- Distant recurrence common (30-50%)
- Adjuvant therapy has not been shown to definitively improve survival