
Thymic Tumors
Author: Paul Schipper, MD
Institution: OHSU
Date Reviewed: March 2025
Original Case: David Mauchley, MD
Learning Domain: General Thoracic
Learning Objective: Management and staging of thymic tumors
PowerPoint File: Thymic Tumors
Case #1
48 yo presents to your office with the following statement, “my primary care doctor said I have a benign thymoma and sent me to you to have it removed. If it is truly benign, why do I need surgery?”
How do you answer this question?
The diagnosis “benign thymoma” does not exist and was a misconception, possibly due to sometimes very slow growth. All thymomas have the possibility of spread, most often local or local-regional.
Histological Classification
- Cytologically Bland Thymomas (“benign” thymomas)
- Cytologically bland cells, little to no atypia
- Best prognosis
- Majority of thymic tumors
- Well-differentiated thymic carcinoma
- Mostly bland but evidence of invasion
- Thymic Carcinoma
Case #1
- Once past the first question, you take a history.
- What symptoms would you expect her to have, assuming she does indeed have a thymic tumor?
- She reports vague chest discomfort and an occasional cough that she thinks has gotten worse over the last several months. Otherwise asymptomatic.
- What might you ask about in her PMH?
Question #1
Next to Myasthenia Gravis, what is the second most common parathymic syndrome associated with the presence of a thymoma?
A. Pure red cell aplasia (4%)
B. Cytopenia (15%)
C. Systemic lupus erythematosus (1.2%)
D. Hypogammaglobulinemia (4.5%)
E. Polymyositis (4.5%)
Case #1
- No parathymic syndromes in history.
- Physical Exam is unremarkable.
- What imaging studies would you want to see?
- CT scan, of course.

- Any labs?
- Do you want a biopsy?
- What is the clinical stage of this tumor?
Staging
- Thymic neoplasm have been staged with WHO system, Masaoka System, but no TNM system until…
- Beginning with 8th Edition UICC-AJCC, when a TNM system was introduced.
- As of Jan 2025, the 9th edition TNM staging is used to stage Thymic Epithelial Neoplasms/Tumors, which includes thymoma and thymic carcinoma. Neuroendocrine Tumors of the thymus are also staged with this system, although survival data is still sparse.
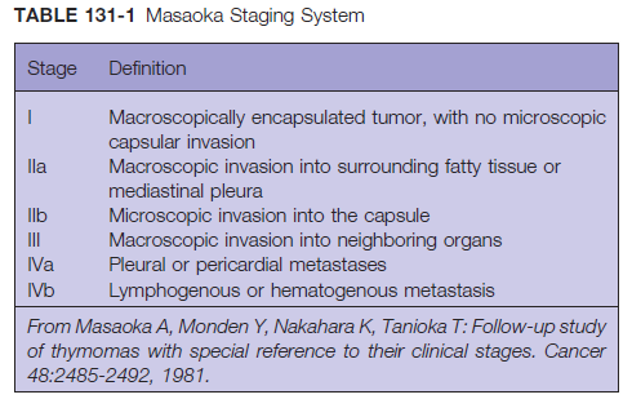
Masaoka Staging System
(for historical use only)
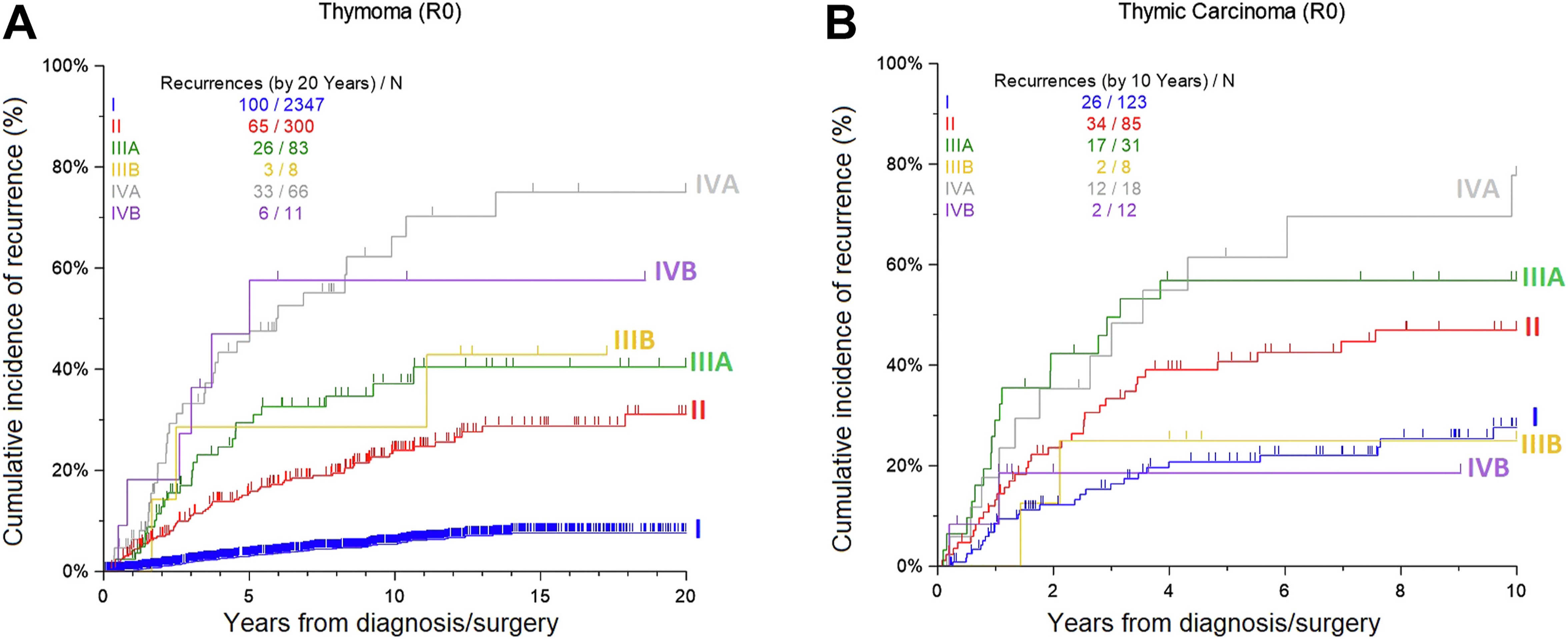
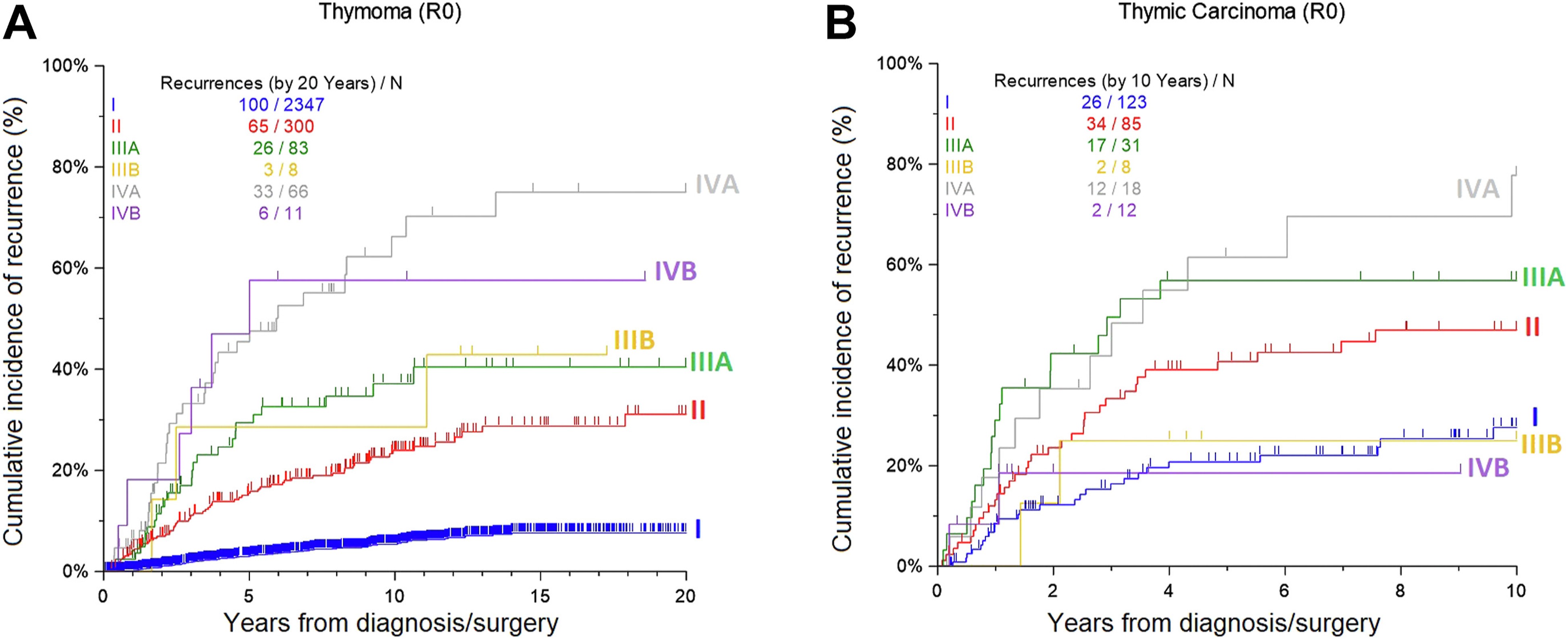
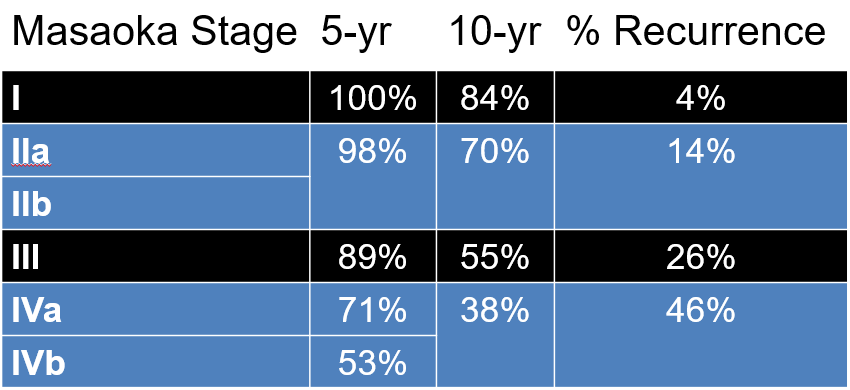
Survival by Masaoka
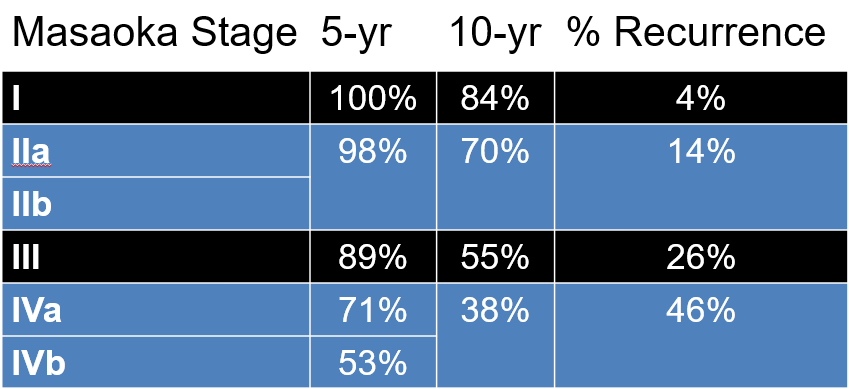
5-yr data: Kondo ATS 2003. 10-yr data: Values represent averages of reported ranges.
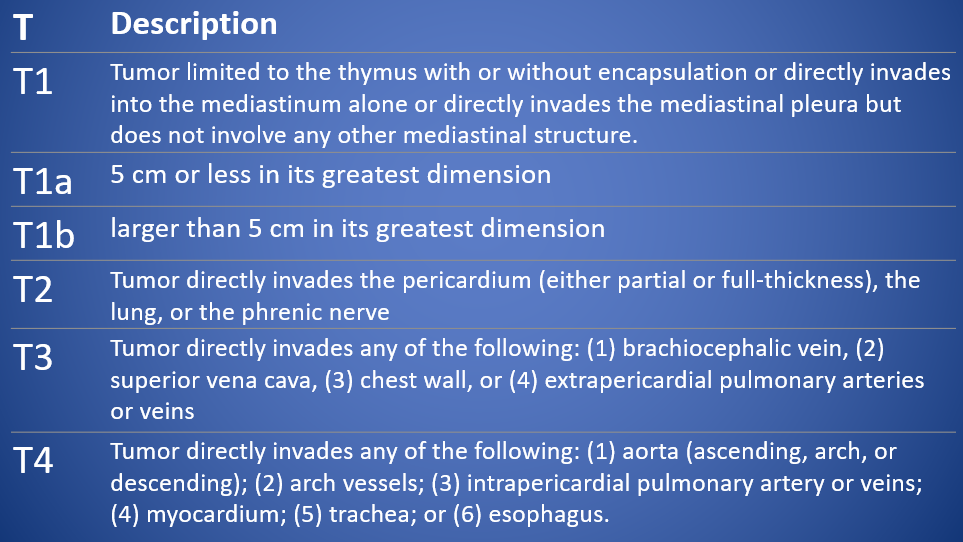
T Descriptor
9th Edition Thymic Epithelial Neoplasms (Thymoma and Thymic CA)
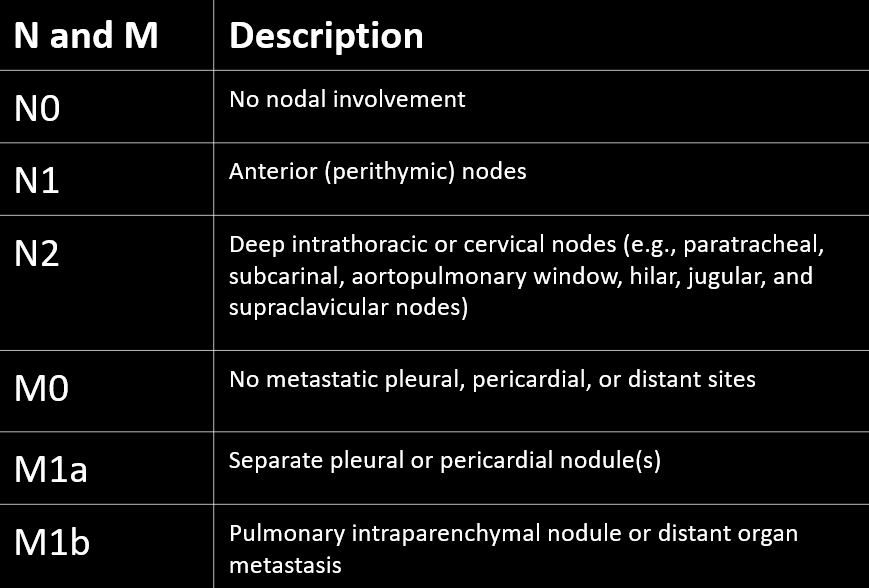
Nodal and Metastasis Descriptors
9th Edition Thymic Epithelial Neoplasms (Thymoma and Thymic CA)
9th edition TNM Staging
Thymic Epithelial Neoplasms
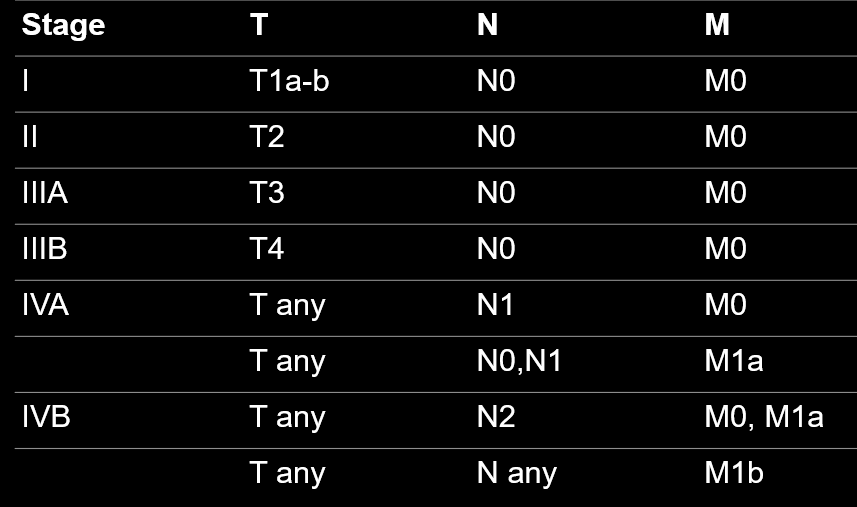
Journal of Thoracic Oncology, Volume 18, Issue 12, 2023, Pages 1655-1671
Case #1
How do you plan on treating this tumor?
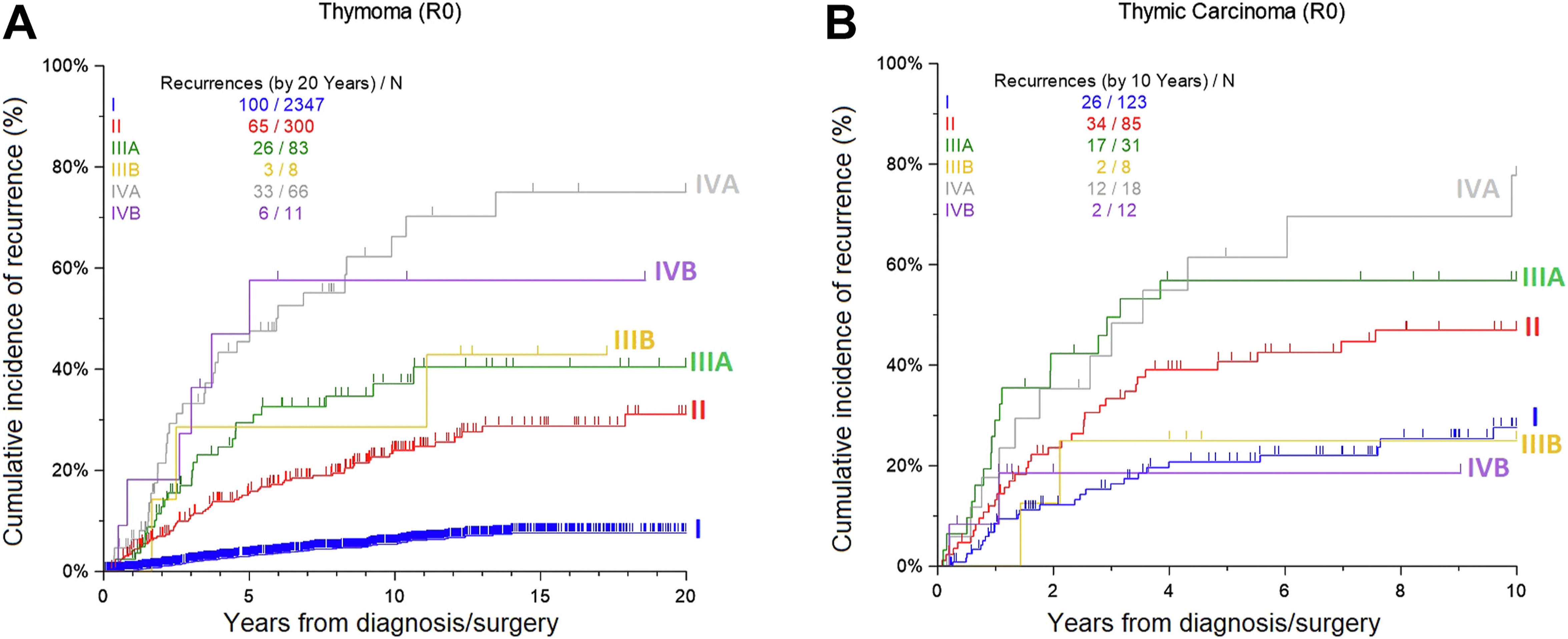
The patient agrees to have surgery, but now that you’ve explained to her that the diagnosis of benign thymoma doesn’t exist, she wants to know if this tumor is likely to “do her in.” What do you tell her?
Question #2
Which of the following prognostic factors have consistently been shown to predict better survival in the treatment of thymic tumors?
A. Histologic type
B. Male sex
C. R0 resection
D. Early stage
E. Presence of Myasthenia Gravis
Case #1
How do you plan on approaching this tumor surgically?
- You do a thymectomy, she recovers well, path shows a cytologically bland thymoma with microscopic invasion into the tumor capsule (T1aN0M0, Stage Ia Thymoma)
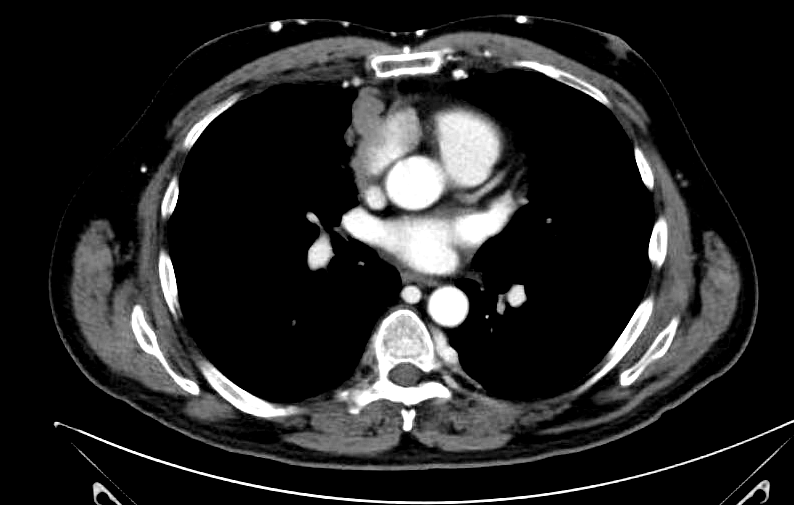
- 5 years later, she returns to your office with the following CT scan
What do you do with this?
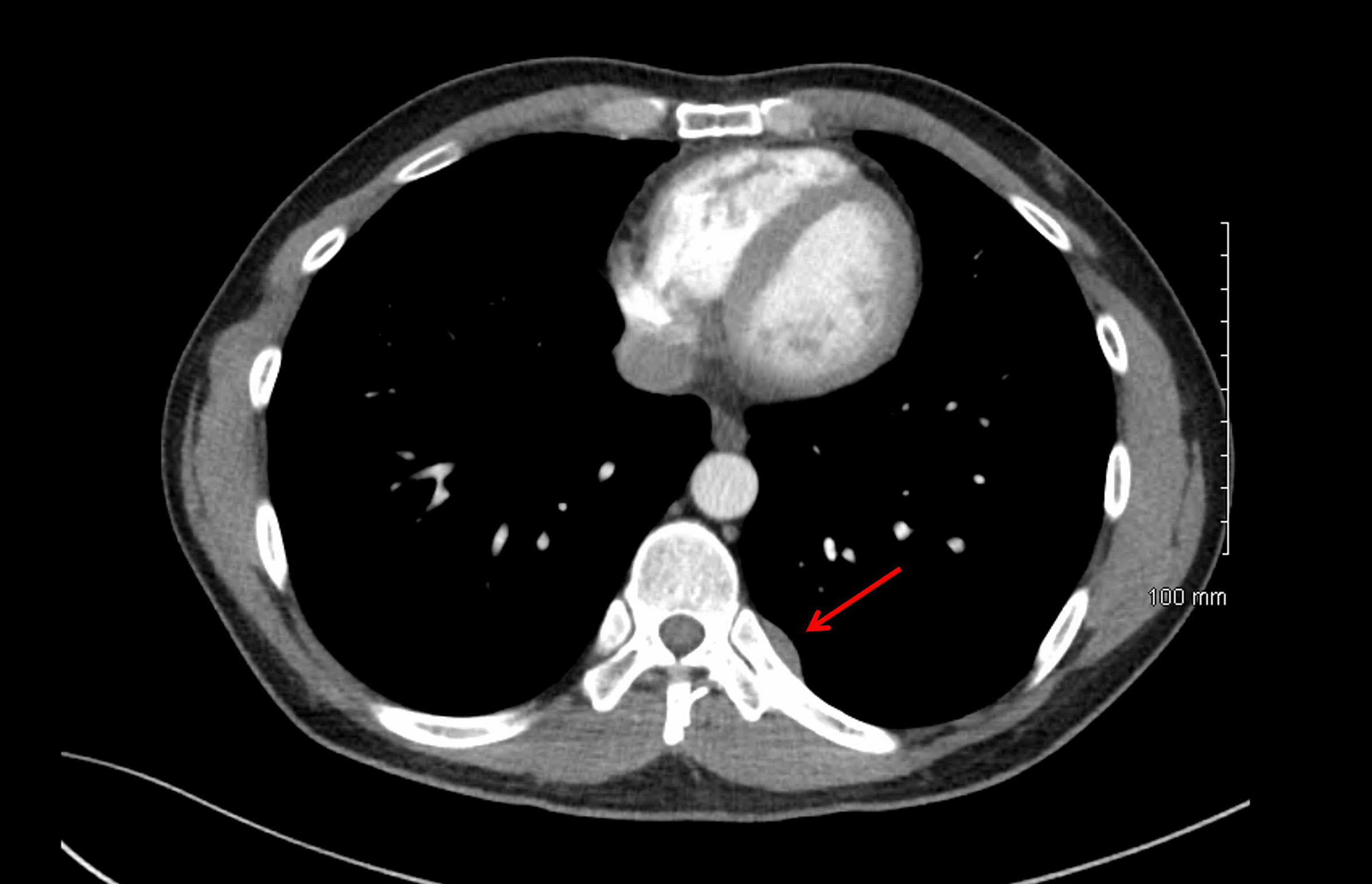
What is the stage?
- This is a separate pleural nodule = M1a, Stage IVA.
- Incorporating the original tumor, T1aN0M1a, Stage IVA
- The pleural nodule is now driving the prognosis.
Treatment of Recurrence
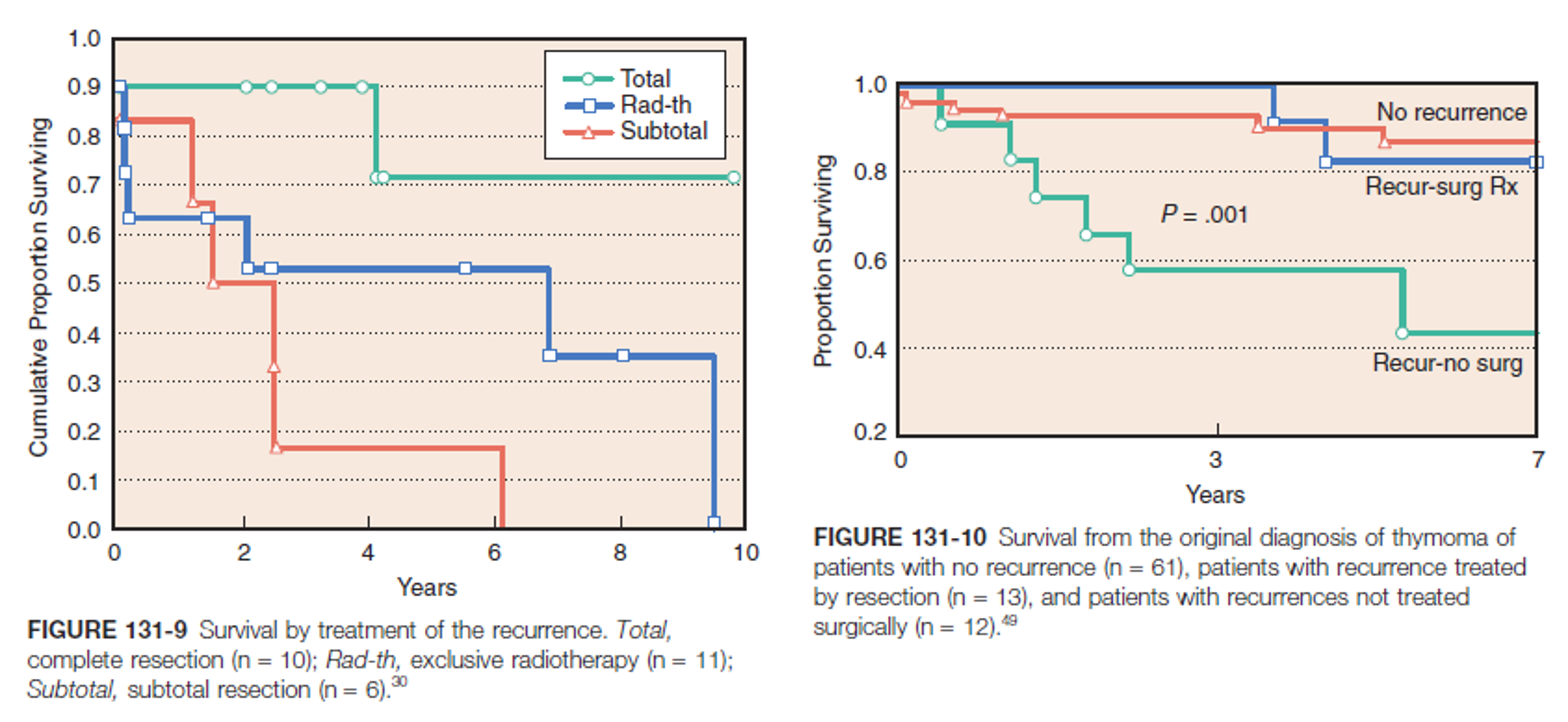
If complete resection can be achieved, it is the best option.
Case #2
45 yo M with well controlled MG presents with new onset and progressive facial flushing, particularly when he leans forward.
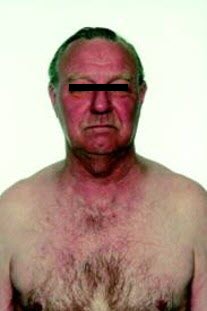
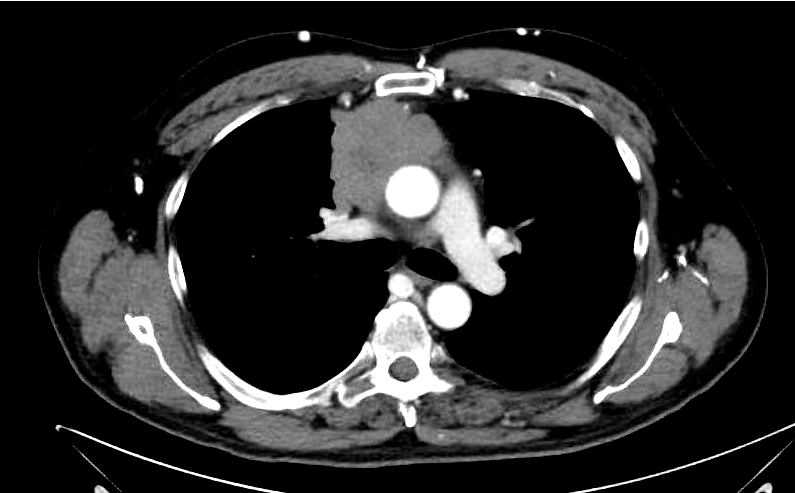
What is the facial flushing/discoloration?
- Look at the tumor location
- What does the tumor stenose/compress
- The Superior Vena Cava is compressed
- He has Superior Vena Cava syndrome from a compressive anterior mediastinal mass.
Do you want a biopsy?
- Biopsy shows lymphocyte rich thymoma
What would your initial management strategy be (remember predictors of survival)?
- Neoadjuvent chemotherapy
- Thymoma has very high response rate to chemo
- Typically cisplatin, doxyrubicin, cyclophosphamide
- Improves chance of R0 resection in stage III and IV tumors
He completes neoadjuvant therapy and his flushing improves. Restaging CT scan shows regression of the tumor.
- What incision are you going to make?
On exploration, you find that the tumor involves the R phrenic nerve and is inseparable from the ascending aorta.
- What now?
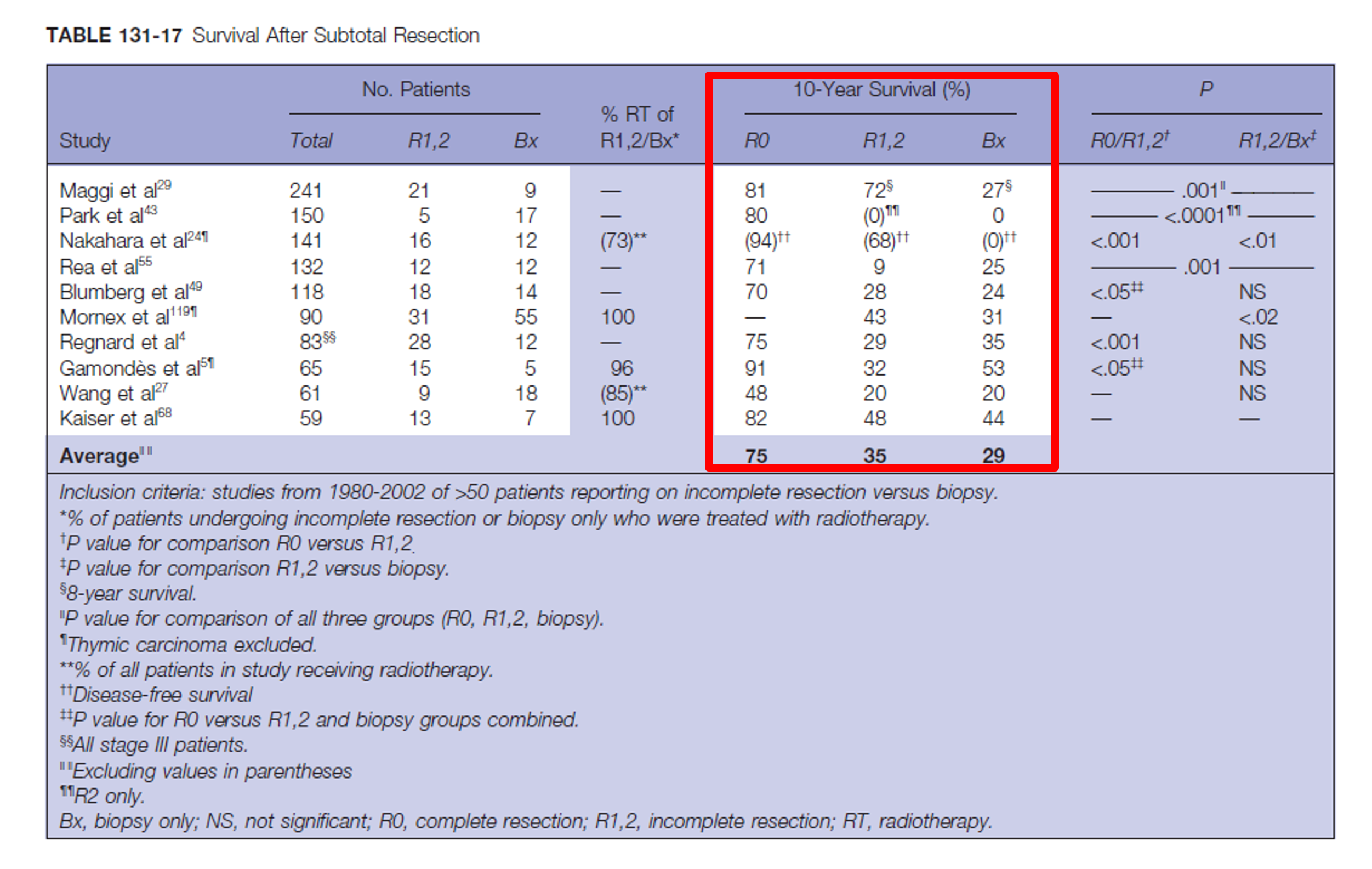
Role of Partial Resection
- Data aren’t entirely convincing
- Partial resection seems to have slight survival benefit over biopsy alone
- Local recurrence is lower in R1 resection compared to R2 (adj radiotherapy)
Learning Points
- Surgery is mainstay of therapy for thymic tumors
- R0 resection should be achieved if possible
- Most important prognostic factors are stage and completeness of resection
- There is no such thing as a benign thymoma
- Biopsy of presumed thymoma is not detrimental
- Neoadj chemotherapy for advanced stage thymoma appears to improve survival and resectability
- Adjuvant radiotherapy is indicated in patients with incomplete resection
- Resection of recurrent thymoma should be done whenever possible