
Thoracic Surgery General Management I
Author: Brian Mitzman, MD
Institution: University of Utah
Date Reviewed: March 2025
Original Case: Stephen Yang, MD; Johns Hopkins University
Learning Domain: General Thoracic Surgery
Learning Objective: Lung anatomy and management
PowerPoint File: ![]() TS01 - Gen Management I.pptx
TS01 - Gen Management I.pptx
Discussion Questions
- Most common anomalies of the lung?
- Encountered during bronchoscopy?
- During lobectomy of individual lobes?
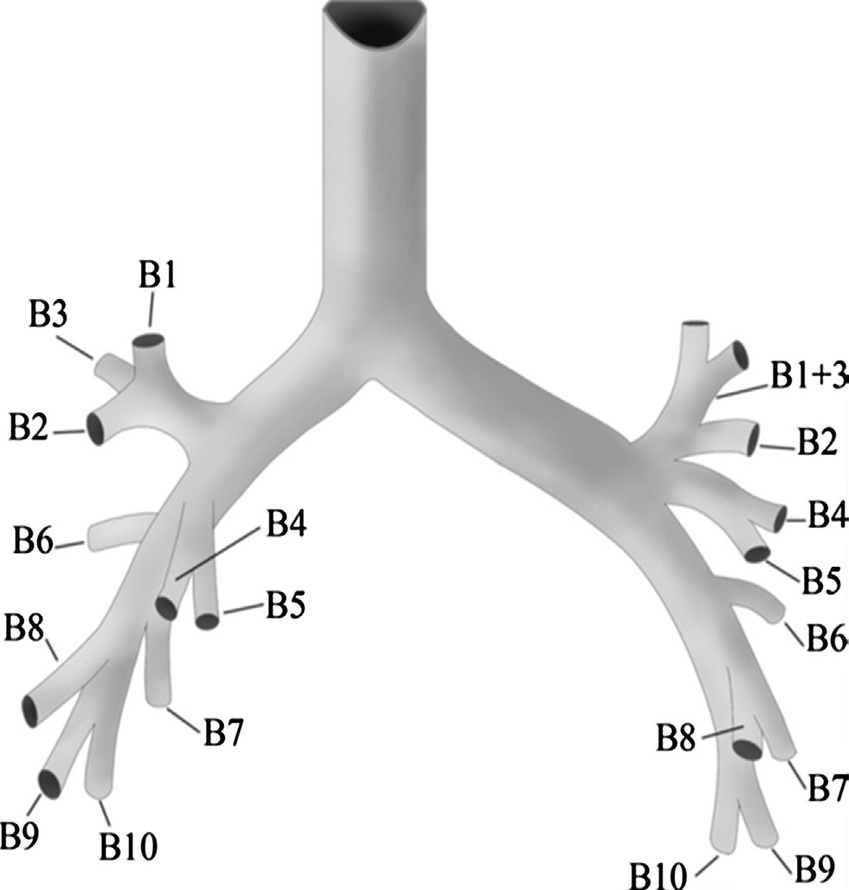
Standard Anatomy - Boyden Classification
Bronchopulmonary segments shown. Each tertiary bronchus is numbered with respect to its position in the matching numbered bronchopulmonary segment.
a) Right lung (lateral view) / b) Right lung (medial view)
c) Left lung (lateral view) / d) Left lung (medial view)
e) Segmental or tertiary bronchi

Case #1
A 25 yo M sustains a bullet wound that enters the anterior right chest below the nipple and exits below the tip of the right scapula.
- What potential organs are injured?
- What tests or procedures would be done to exclude injuries?
Discussion
- Potential organs injured: lung, esophagus, diaphragm, liver, airway, heart, pericardium
- Work up: FAST, CT chest/abdomen with oral and IV contrast, esophagram, endoscopy (bronchoscopy, esophagoscopy) – depending on situation and acuity
Case #2
- A 68 yo F undergoes an uncomplicated VATS LLL lobectomy
- She is on sips of liquids overnight
- During the first POD1, the chest tube output was 350 cc and serosanguinous
- On POD2, you note that the chest tube output has increased to 750 cc during the 24 hours before and looks turbid
- What is the cause?
- How do you work this up and the treatment?
Discussion
- Differential: Lymphatic leak, chyle leak, esophageal leak
- Workup: Send fluid for triglyceride, chylomicrons, amylase
- Management: Make strict NPO vs chyle-leak diet
Case #2 Outcome
- TG 735 in the chest tube fluid
- PT made NPO > 700 cc/day for ensuing 4 days
- Now what?

Case #2 Outcome
- Percutaneous lymphoscintigraphy showed normal anatomy and leak in subcarinal area
- Output slowed after test to 200/day
- Started on PO diet but output increased to 900 cc cloudy fluid
- Now what?
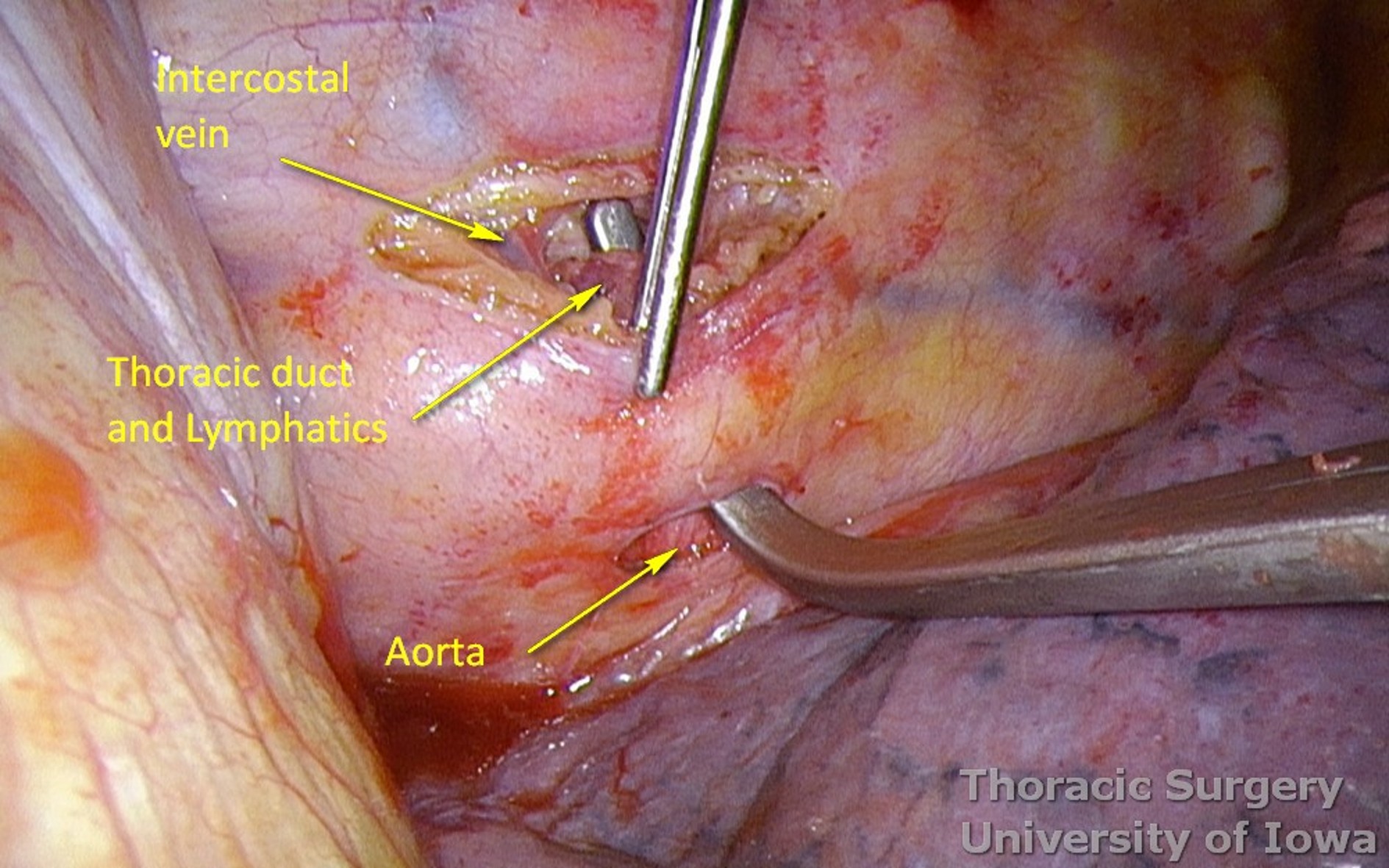
Thoracic Duct Lymphangiogram
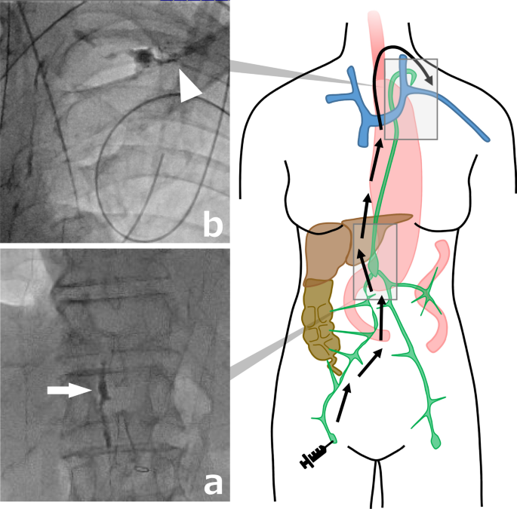
Case #2 Outcome
- PT given regular diet, NPO after midnight
- Right VATS thoracic duct ligation at T10 and T11 level
- Can give intraoperative heavy cream to exacerbate leak for localization
- Drainage stopped intraoperatively
- PT d/c home POD8
Case #3
- You are doing a lingulectomy for a small peripheral 1.5 cm NSCLC.
- You have already divided the lingular PA and PV branches, and already stapled off the bronchus.
- You reinflate the lung briefly to decide where to divide the lung parenchyma, but find that the lingula still inflates partially.
- Why is this so?

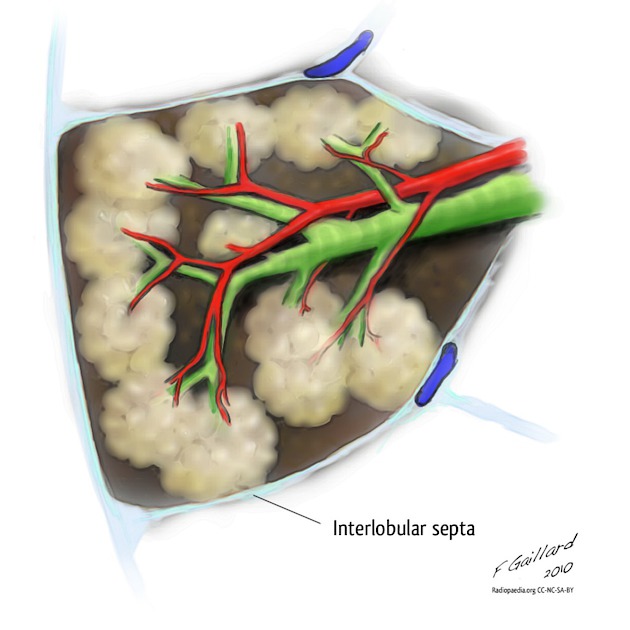
Pulmonary Collaterals: Pores of Kohn
- Interalveolar connections, Canals of Lambert
- Develop after birth
- Account for:
- Ventilation across segments and fissures
- Failure of endobronchial valves
- Local recurrence after wedge resection
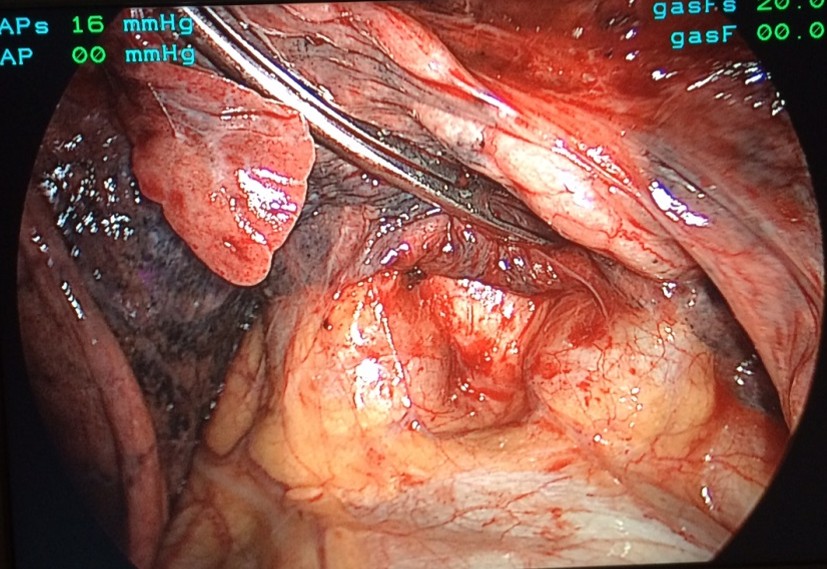
Case #4
- During a difficult left lower lobectomy dissection, you decide to open the pericardium to gain control of the PV.
- You find only one branch emanating from the LA.
- Now what?
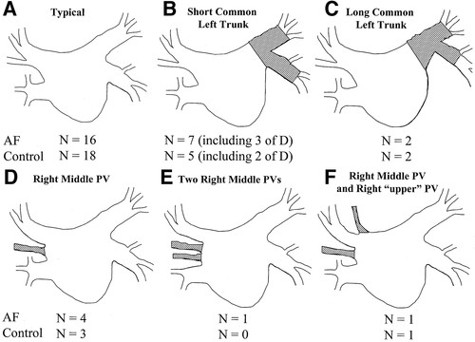
Common PV Trunk
- L>R
- Reported 14% cases
- Always Identify both SPV and IPV
- If accidentally divided, convert to open, reanastomose to LA (not completion pneumonectomy)
Case #5
- A 30-year-old woman presented with a history of two episodes of “pneumonia” and a three-year history of streaky hemoptysis.
- PMH is unremarkable and she is a non-smoker.
- Bronchoscopy reveals erythema of the left lower lobe bronchus and cytologic specimens were negative for malignant cells.
- A CT was obtained (shown).
- What is the diagnosis and treatment?
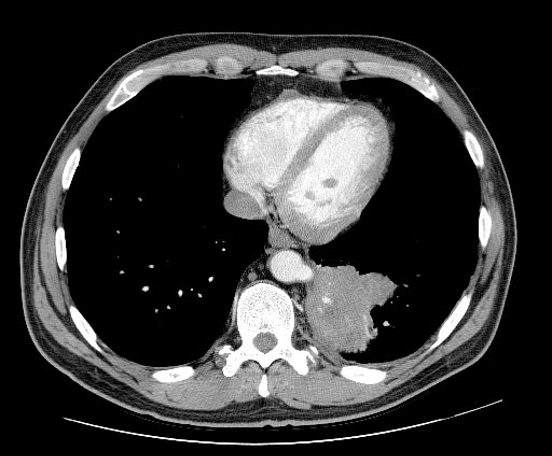
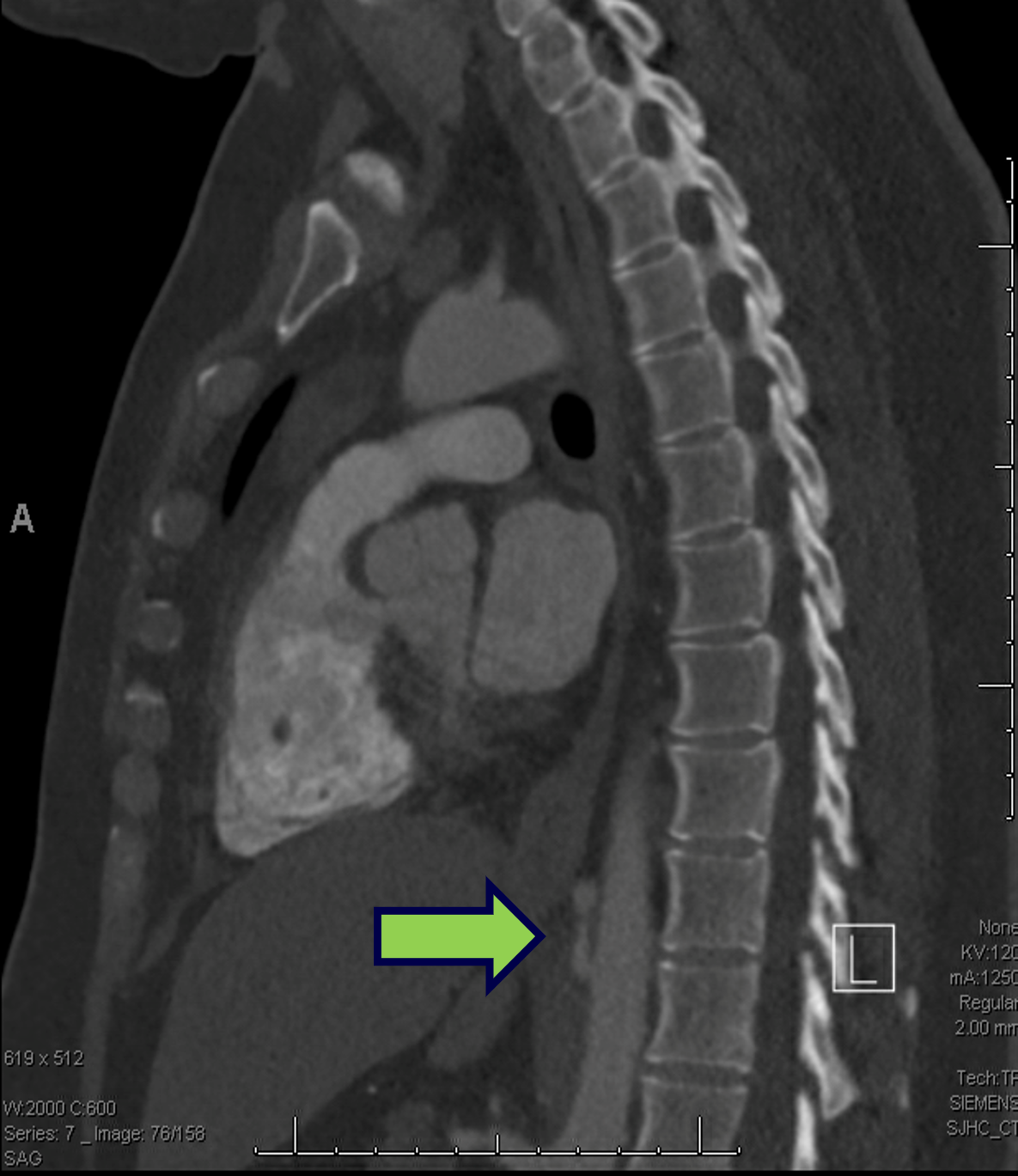
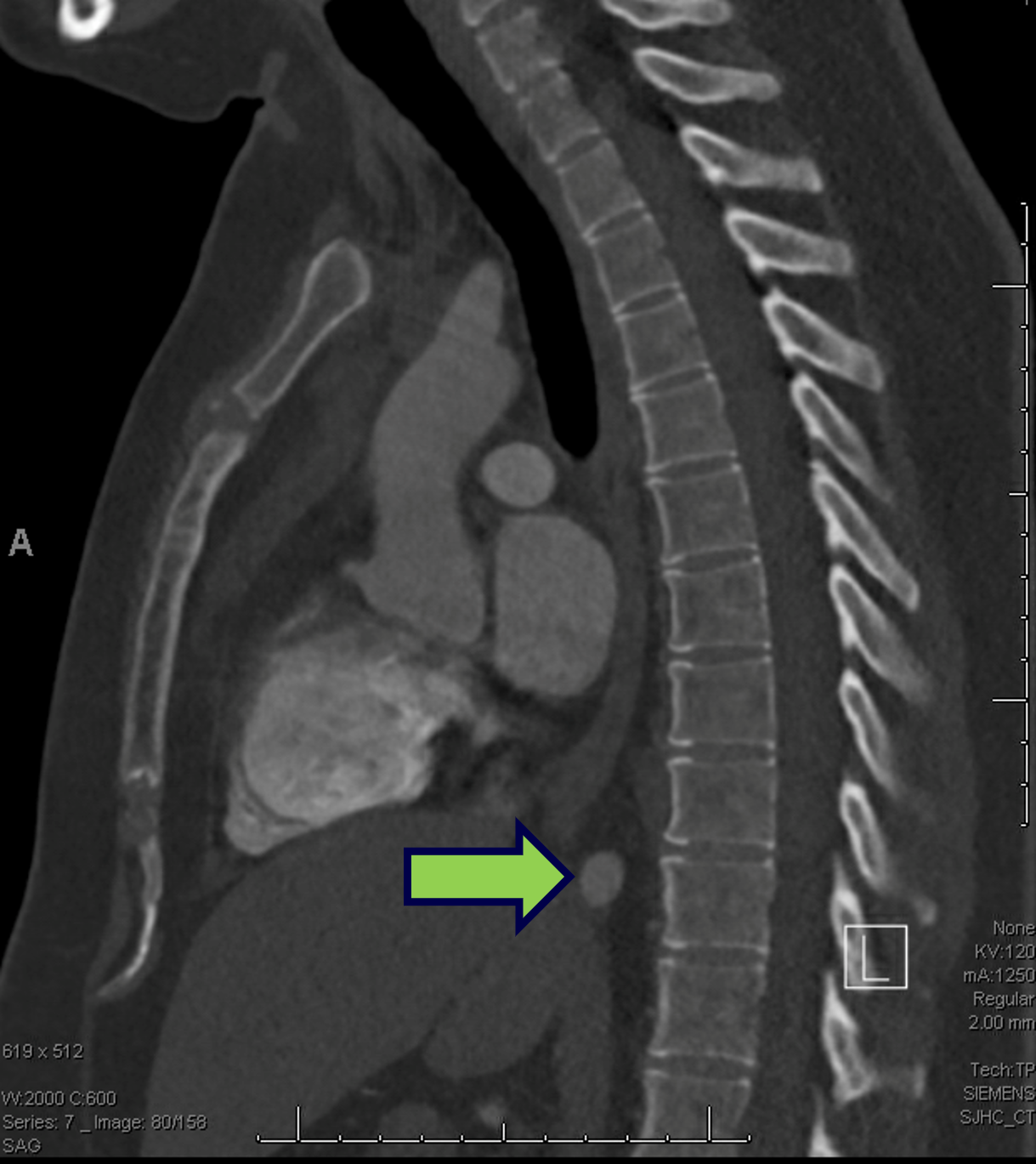

Case #5 Outcome
- Diagnosis of pulmonary sequestration - what type?
- Taken to OR for left VATS resection of sequestrated lung
- Feeding aortic artery found in inferior pulmonary ligament
- Discharged POD 4
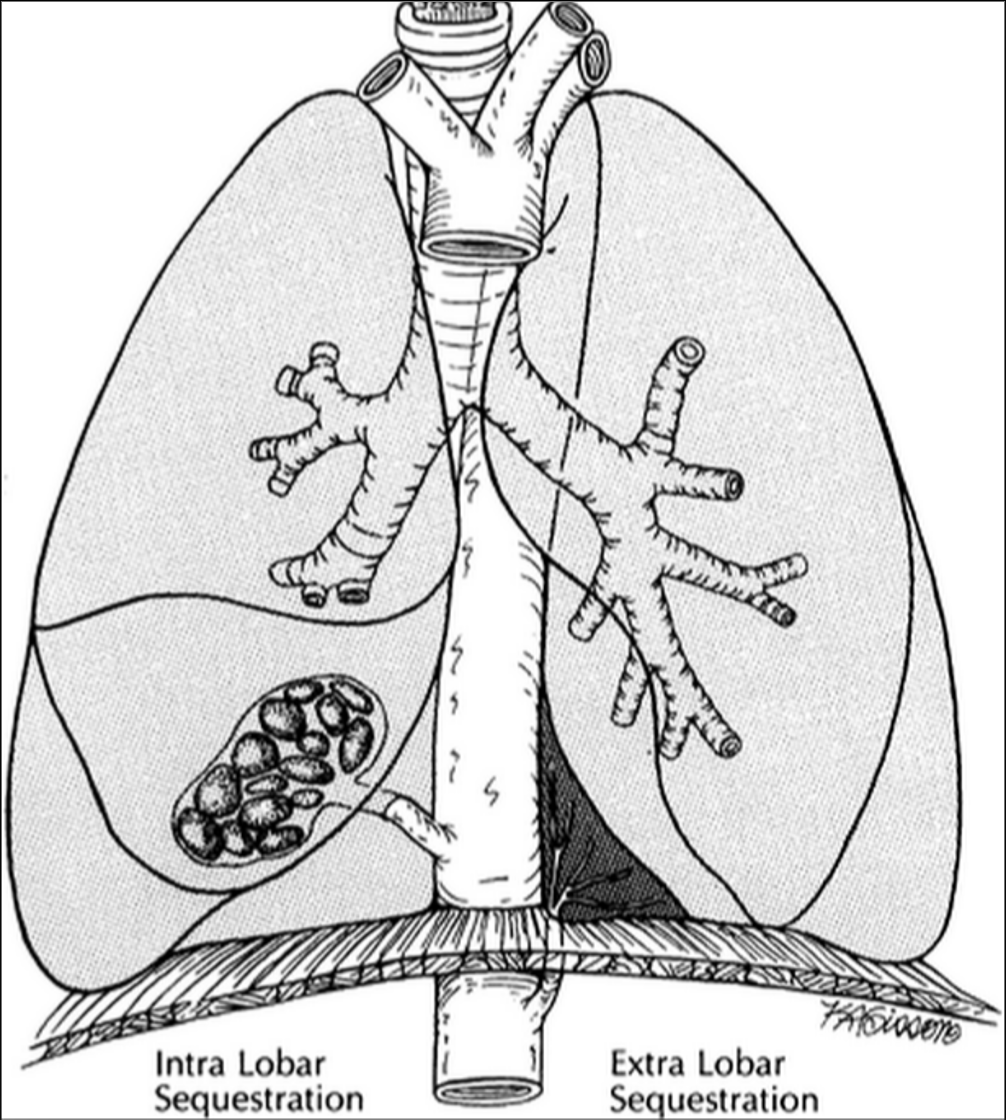
| Intralobar Sequestration | Extralobar Sequestration |
| Shares visceral pleura of normal lung | Locked up within own pleural membrane separate from normal lung |
| Pulmonary venous drainage | Congenital systemic venous drainage |
| Incidence 75% | Incidence 25% |
| Symptoms due to associated anomalies 11%; 85% are asymptomatic | 60% symptomatic 20% asymptomatic |
| Recurrent respiratory infection | Infections rare |
| Malformations with a portion of lung parenchyma separate from normal lobe. No normal communication with tracheobronchial tree and blood supply from systemic artery (aorta) | |
| Congestive heart failure | |
| Surgical resection for symptomatic lesions | |
Case #6
What is this anatomic anomaly?


Case #7
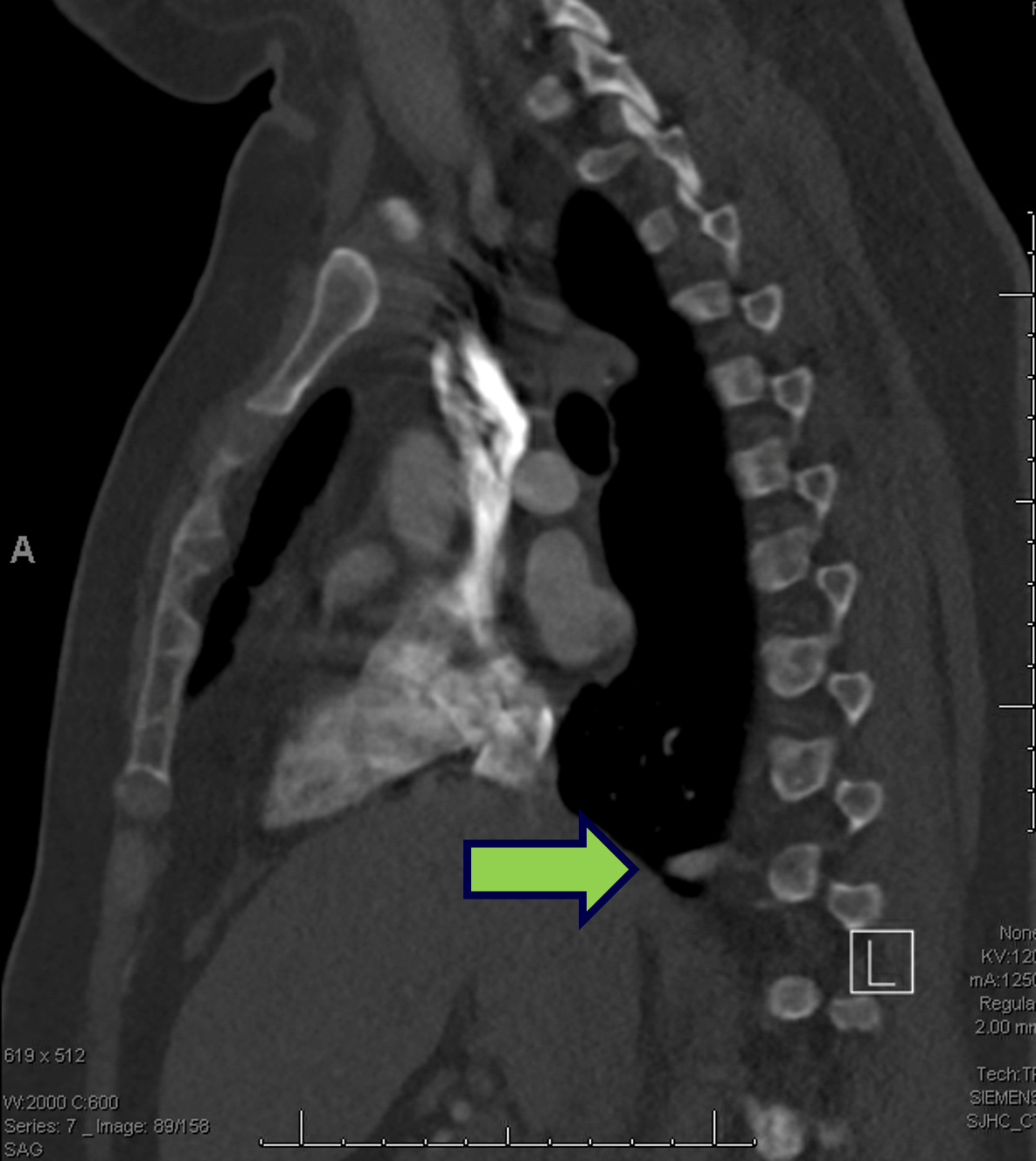
- A 25 year old woman presented with a history of progressive SOB over 3 years. Inhalers do not help her diagnosis of asthma.
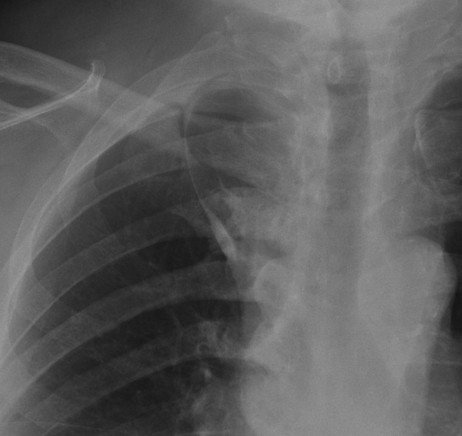
- CXR and CT are shown.
- Her past medical history is unremarkable and she is a non-smoker.
- What is the diagnosis and treatment?
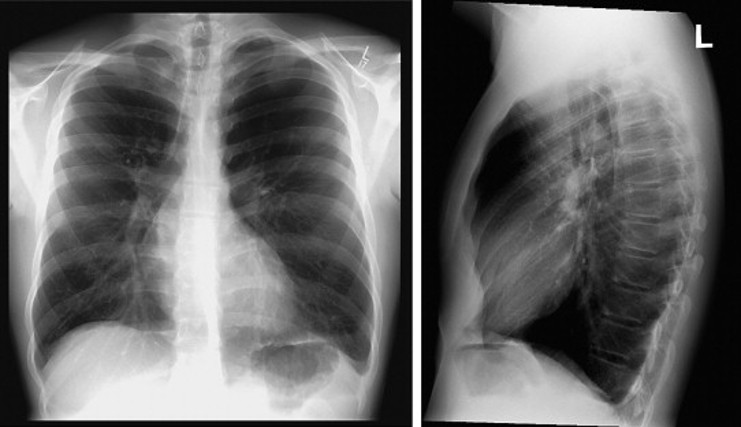

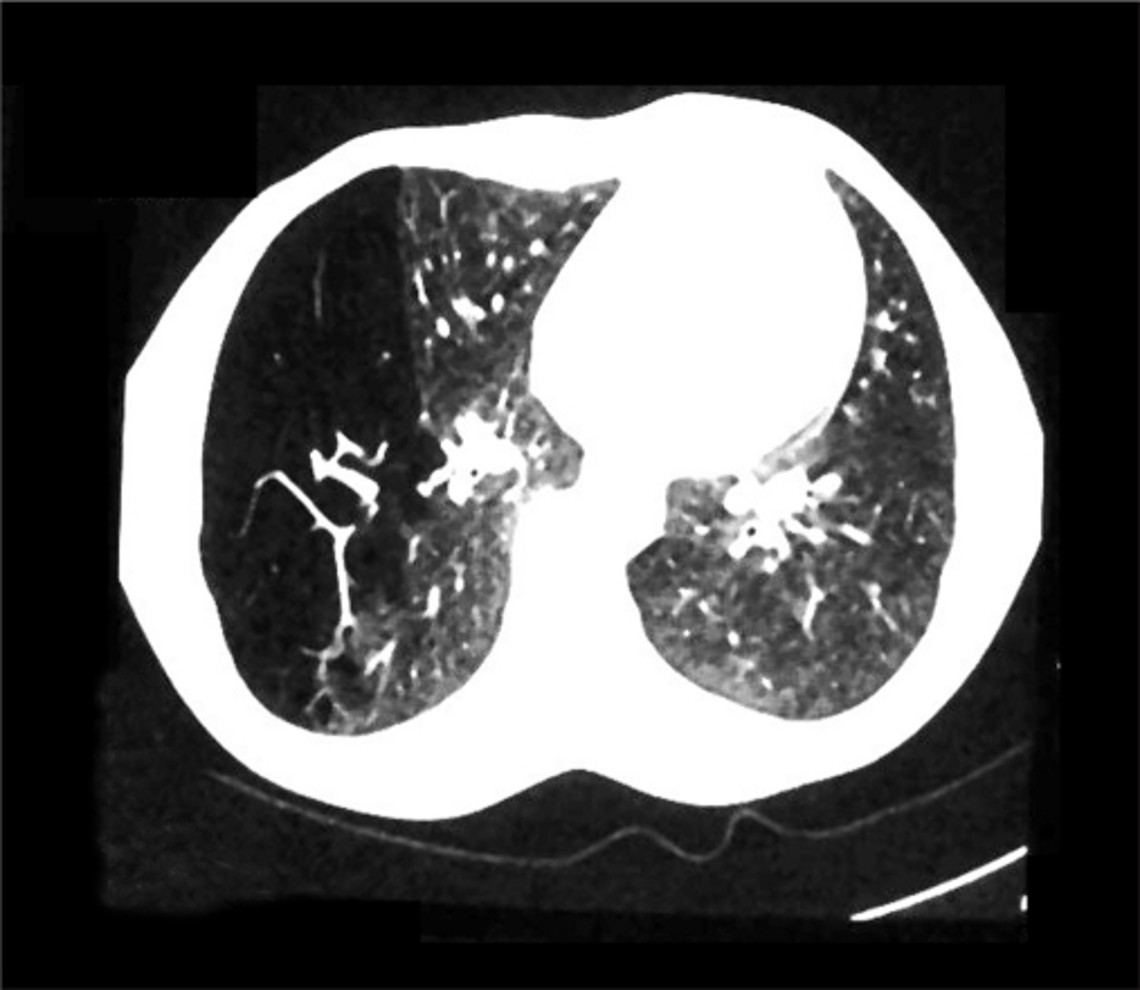
Case Outcome
- Diagnosis of congenital lobar emphysema
- FEV1 68% predicted, DLCO 86% predicted
- Ventilation perfusion scan showed matched defect to RLL
- Underwent right thoracotomy, RLL lobectomy
- Discharged POD 4
Learning Points
- Common anatomic pulmonary arterial anomalies most often in LUL, followed by unusual segmental abnormalities in the RUL post segment, superior segments and lingula
- Lymphoscintigraphy can be therapeutic 50% in stopping chyle leaks
- Pulmonary sequestrations are most common in the left side
- Be aware of other congenital disorders: CAM