Post Operative Management VATS Right Upper Lobectomy
Author: Brian Mitzman, MD
Institution: University of Utah
Date Reviewed: March 2025
Original Case: Junaid Haroon, MD; Rosemary Kelly, MD, Chair, University of Minnesota
Learning Domain: General Thoracic
Learning Objective: RML torsion
PowerPoint File: ![]() TS04 - RML Torsion.pptx
TS04 - RML Torsion.pptx
Case History
73 yo RIGHT upper lobe nodule (14mm) on screening CT chest
- PMHx: HTN, Peripheral Arterial Disease, Abdominal Aortic Aneurysm
- PSHx: Knee surgery
- Meds: Albuterol, Amlodipine, Lisinopril, Naproxen, Tamsulosin
- Social: Veteran, current smoker, 75 pack year history, denies ETOH
- Workup:
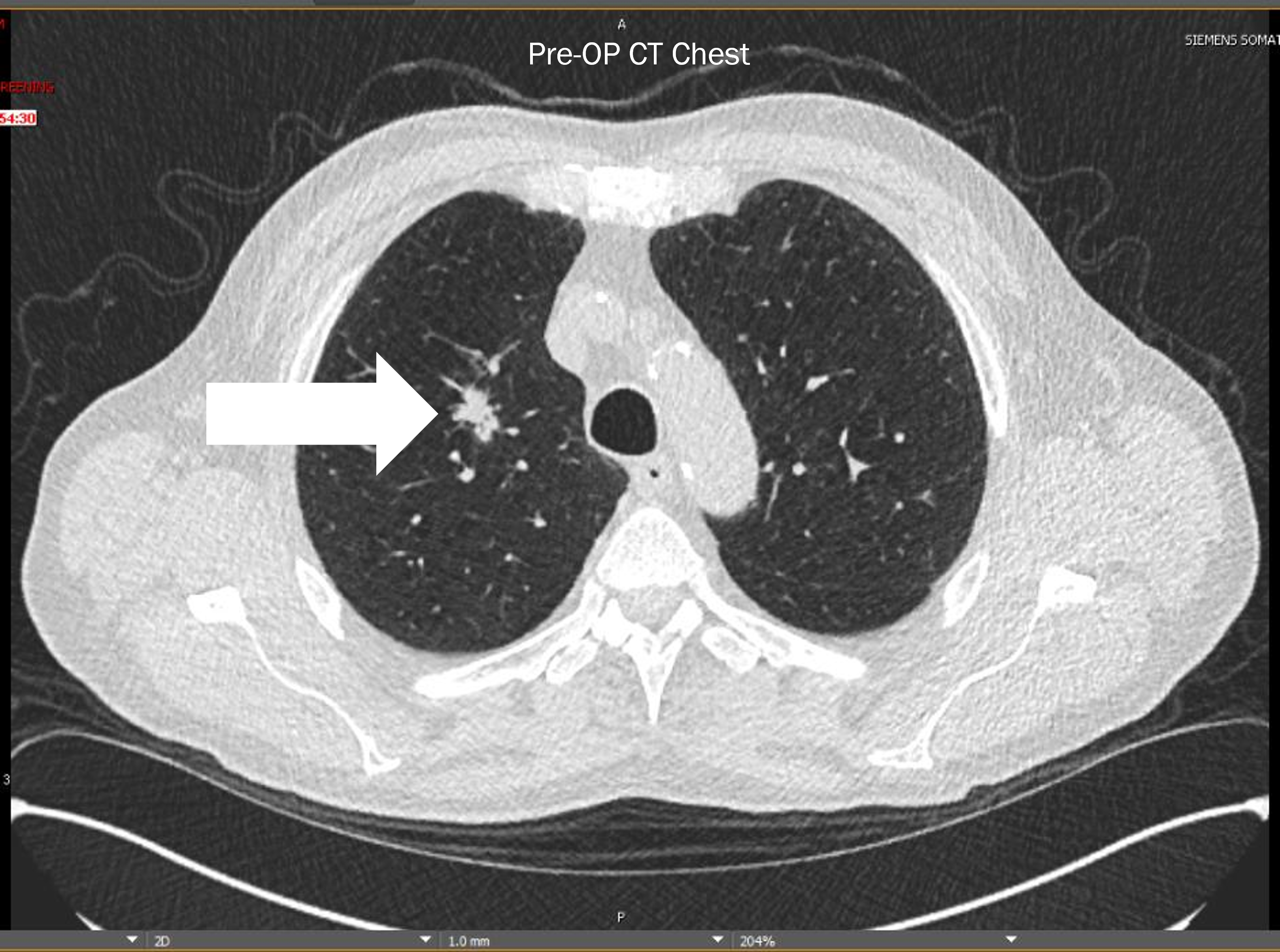
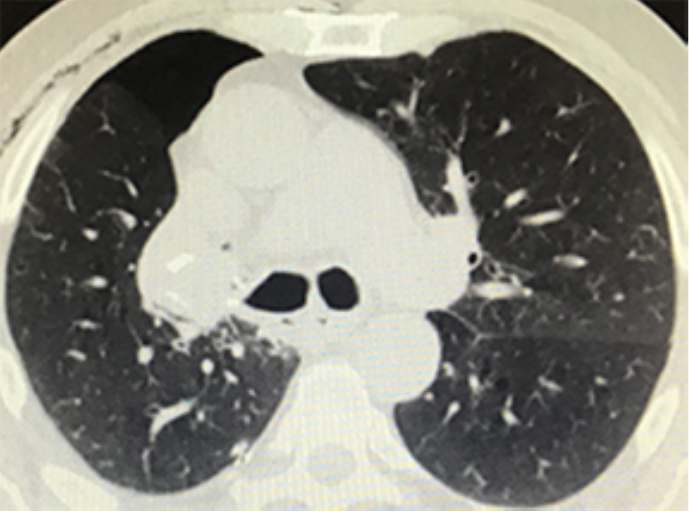
- CT chest: 14mm spiculated nodule
- PET/CT: SUV 6.5
- PFTs: FEV1: 76.9%, DLCO: 60%
- Biopsy: Squamous Cell
Pre-Op CT Chest
Procedure
- VATS Right Upper Lobectomy, Mediastinal Lymphadenectomy
- Complete fissures
- No intraoperative complications
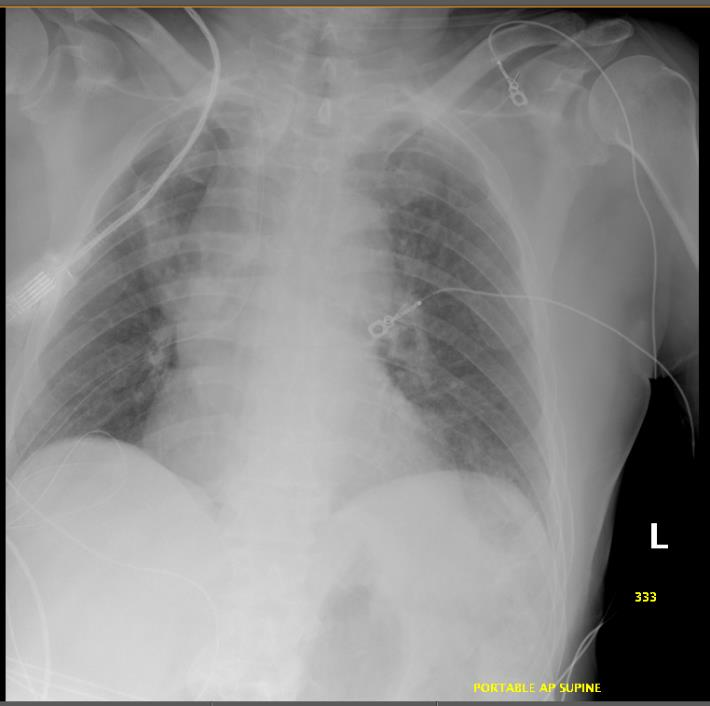
Immediate Post-Op CXR
Hospital Course
- POD 1: Clinically stable
- Afebrile
- Saturating 98% on room air
- In no distress
- Routine CXR done
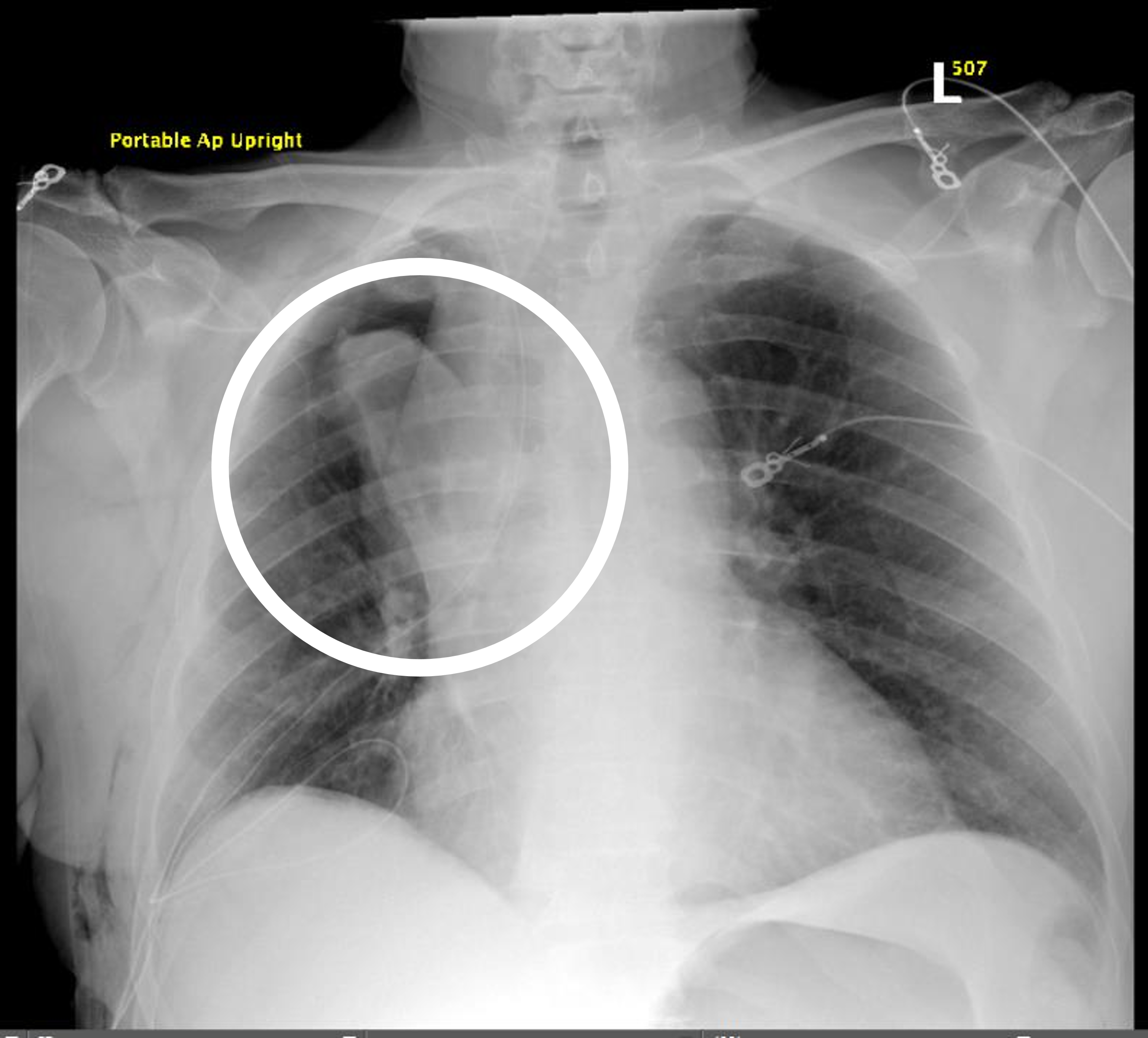
POD 1 CXR
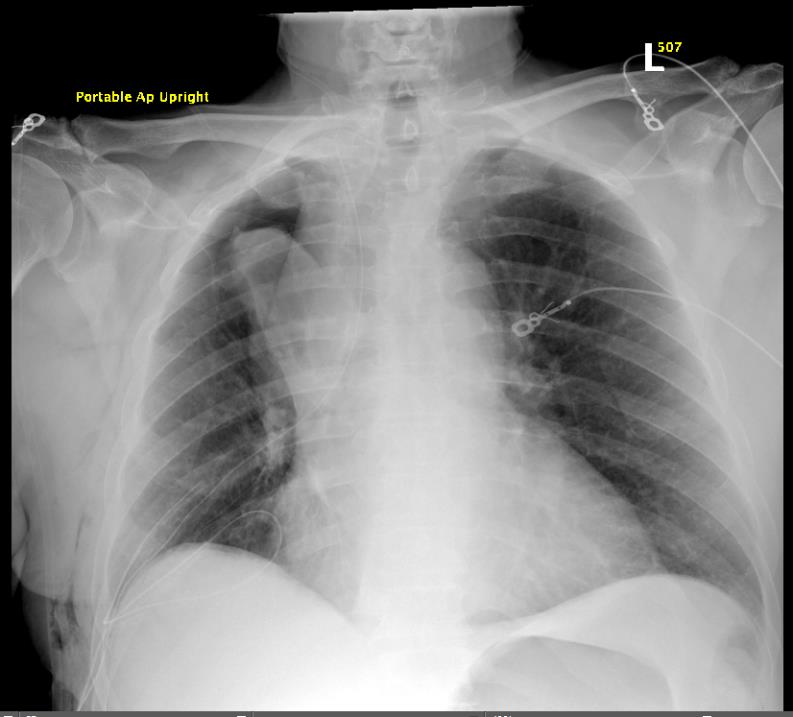
Questions
- What do you see on CXR?
- Differential?
- Next step in care?
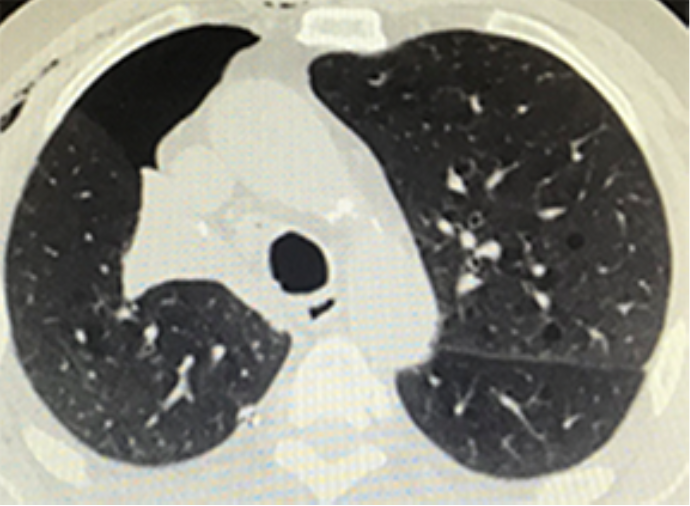
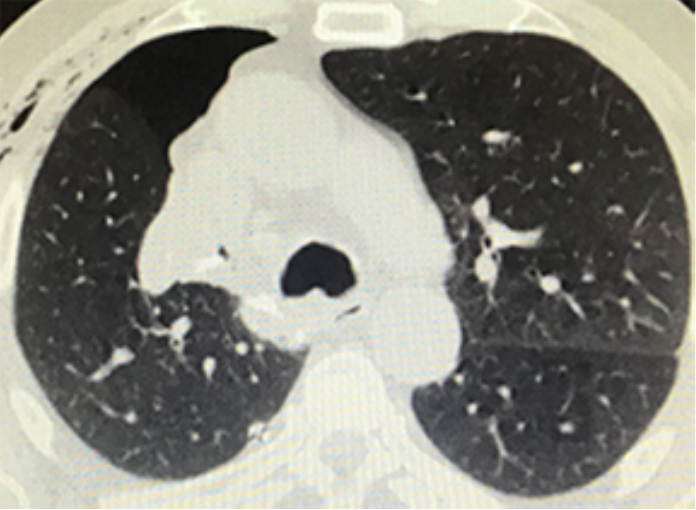
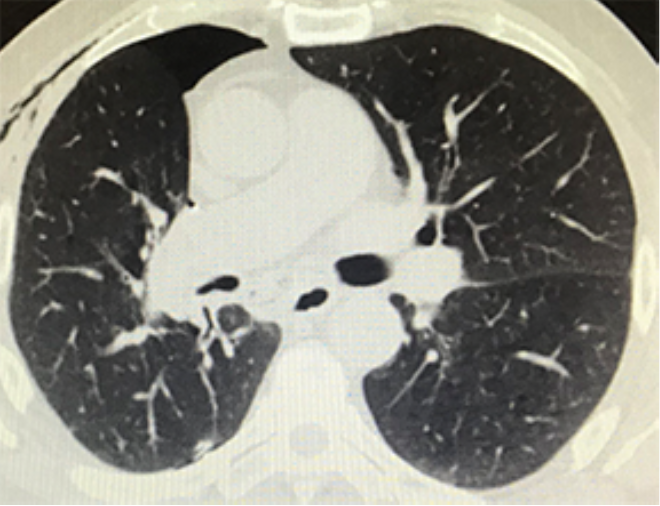
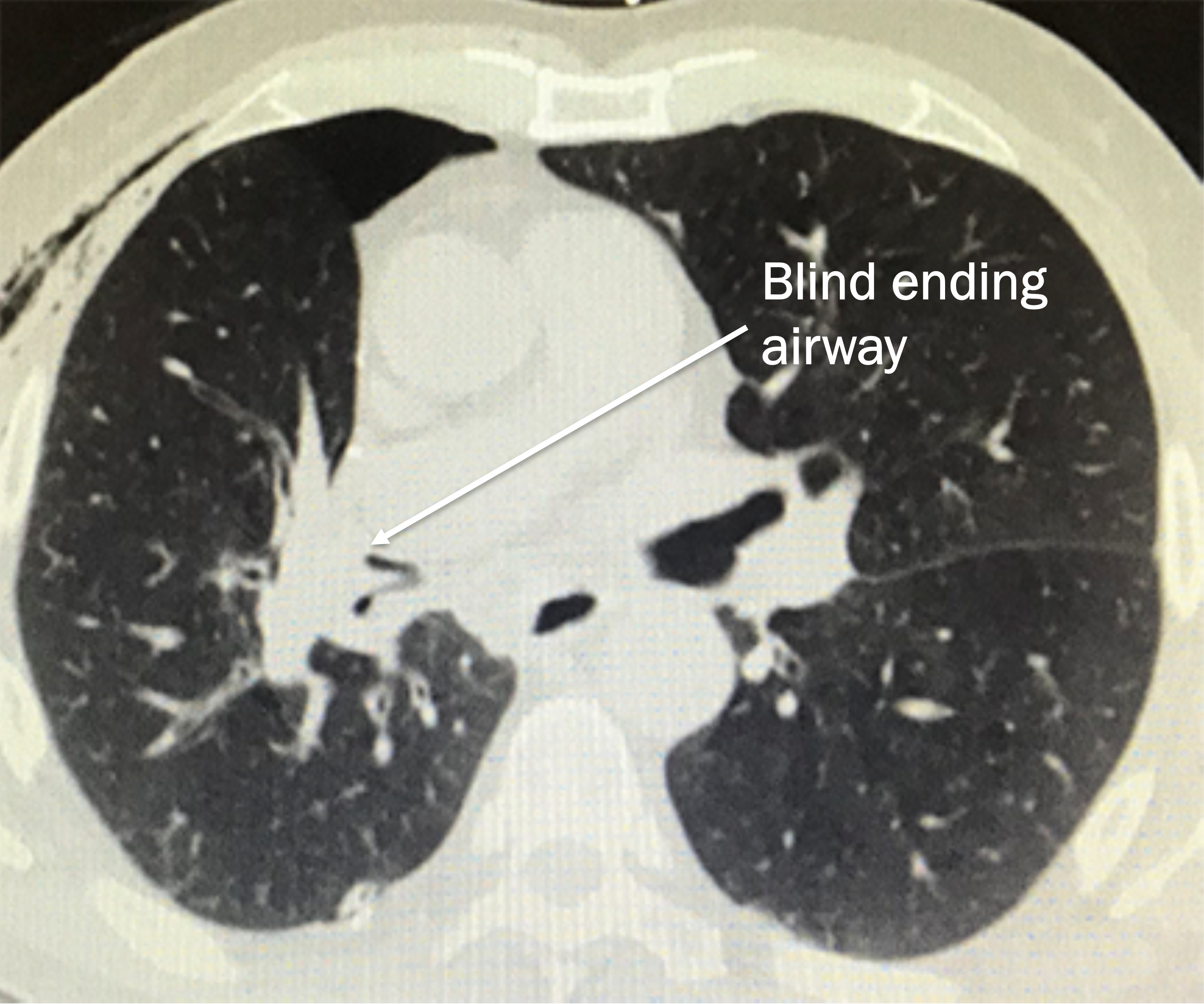
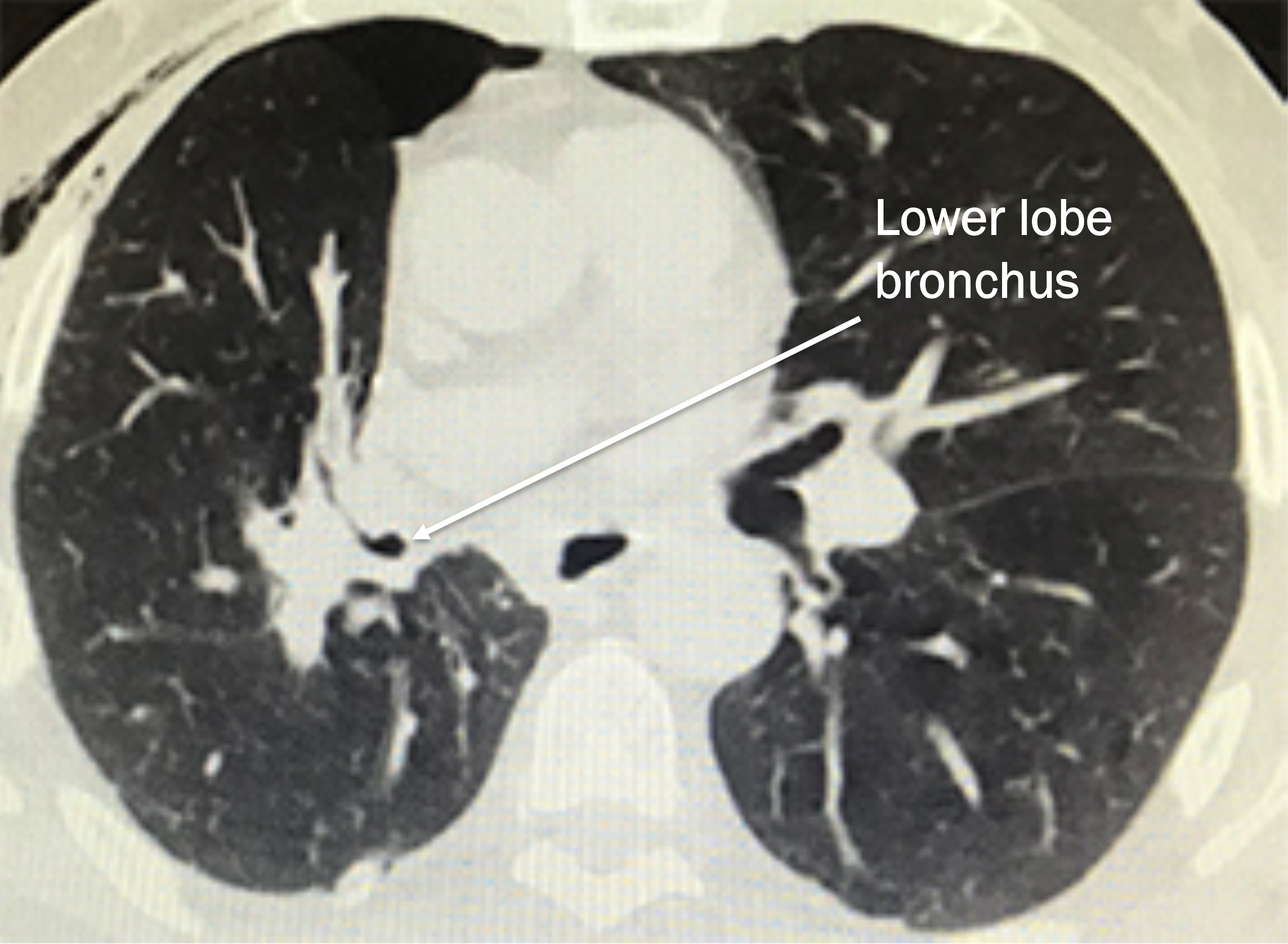
CT Chest
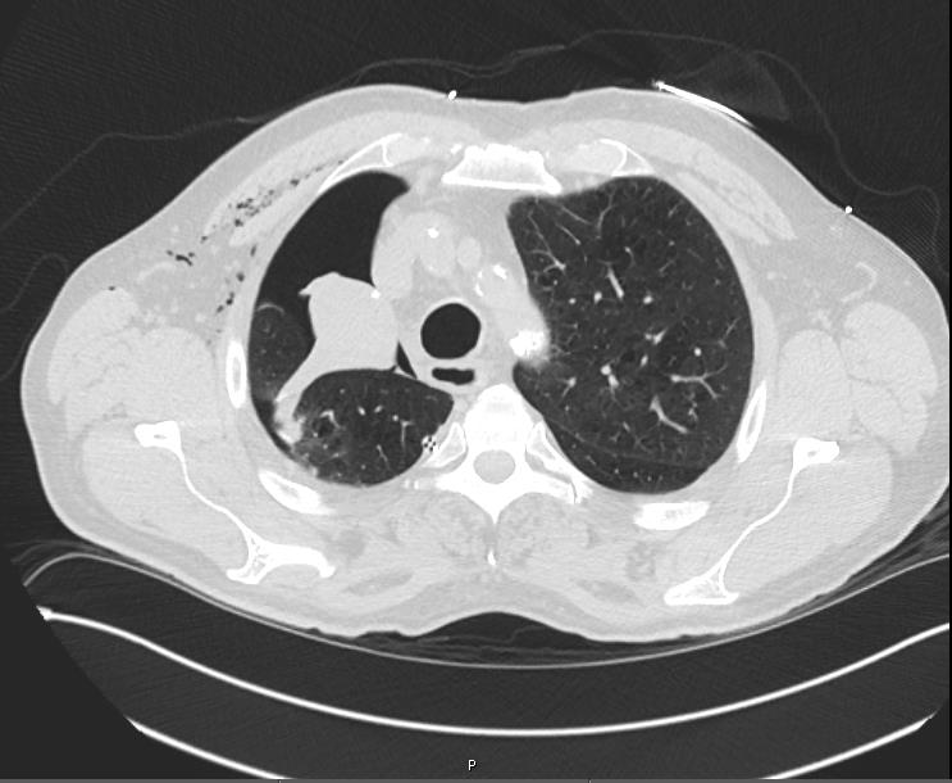

Questions
- What is your differential after CT Chest?
- What other things would you want to look for on the CT Chest that may not be shown?
- Plan?
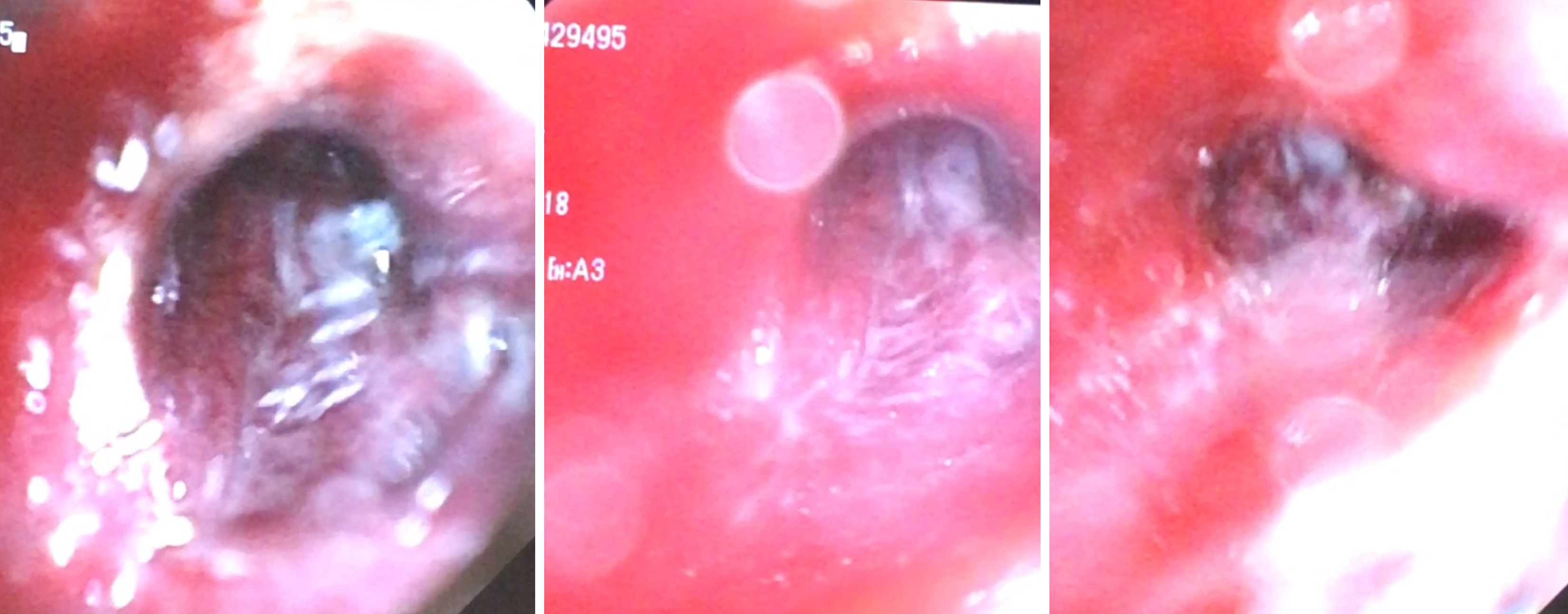
Bronchoscopy
- What are the usual bronchoscopic findings for middle lobe torsion?
- How do you rule out torsion versus mucous plug?
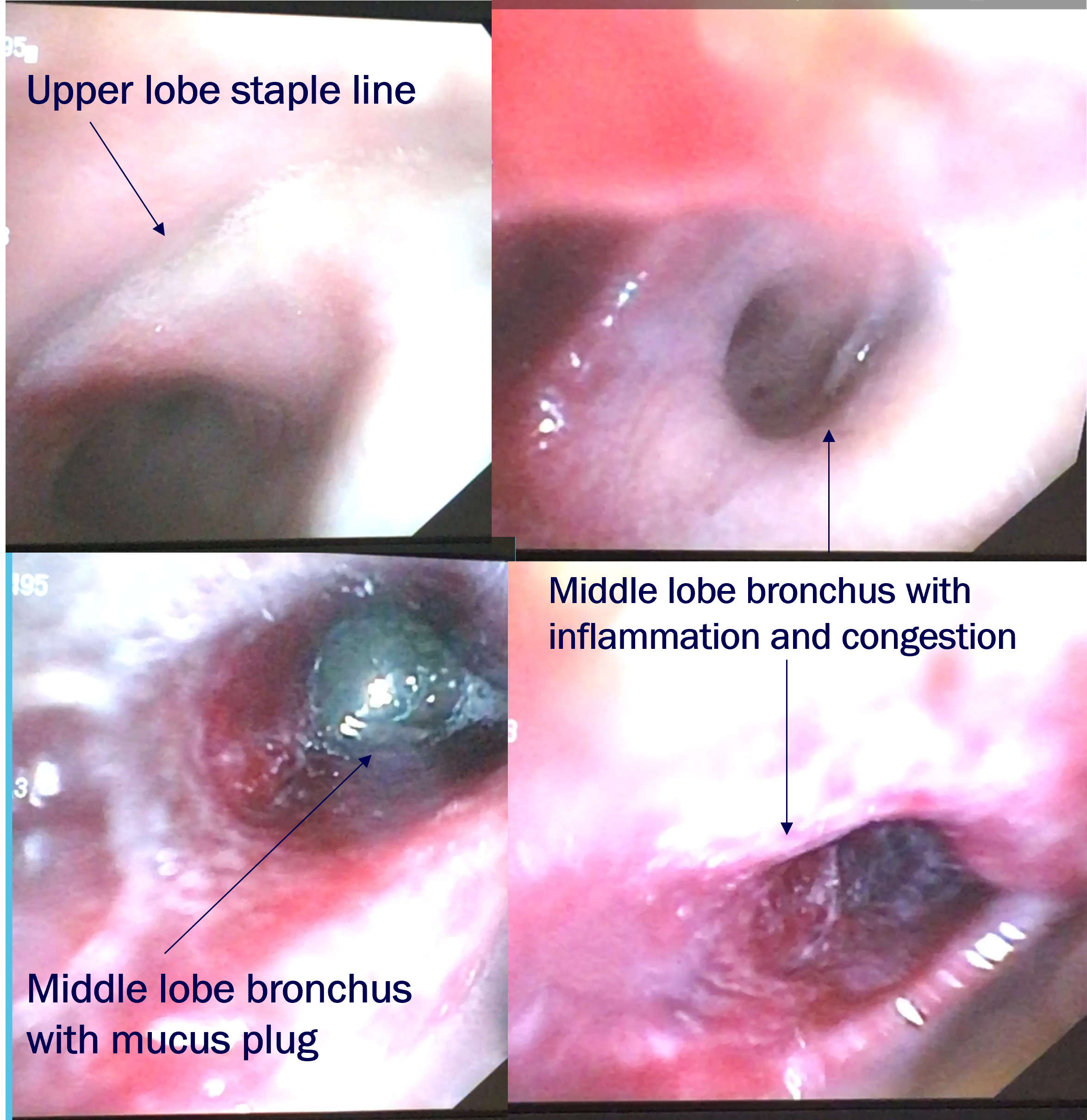
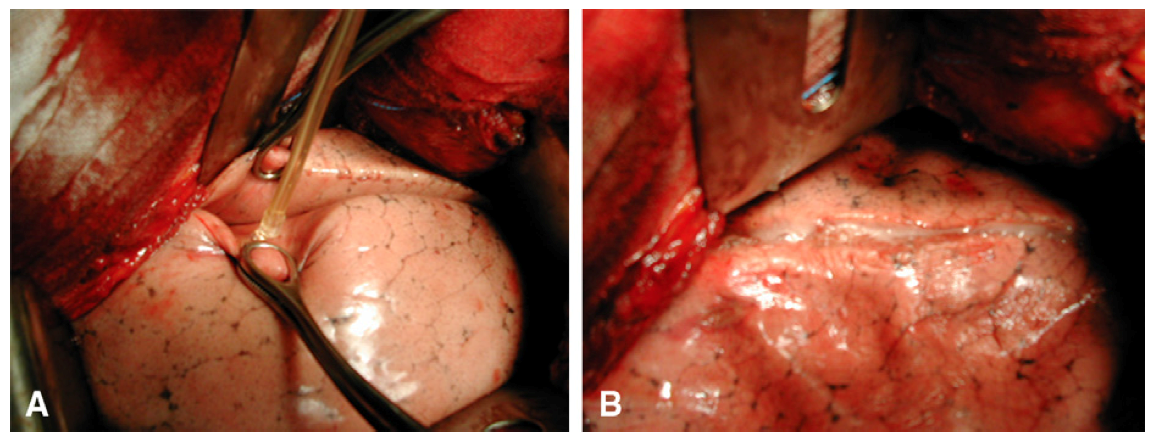
Bronchoscopic view of middle lobe bronchus, after removing mucus
Hospital Course Part 1
- CT Chest:
- Mucus plugging with collapse of Right middle lobe
- Bronchoscopy
- Rt upper lobe bronchial stump intact
- Rt middle lobe bronchus with mucus plugging
- Once mucus plug removed, bronchus appeared congested and inflamed
- Unable to pass scope into slit like opening of middle lobe bronchus
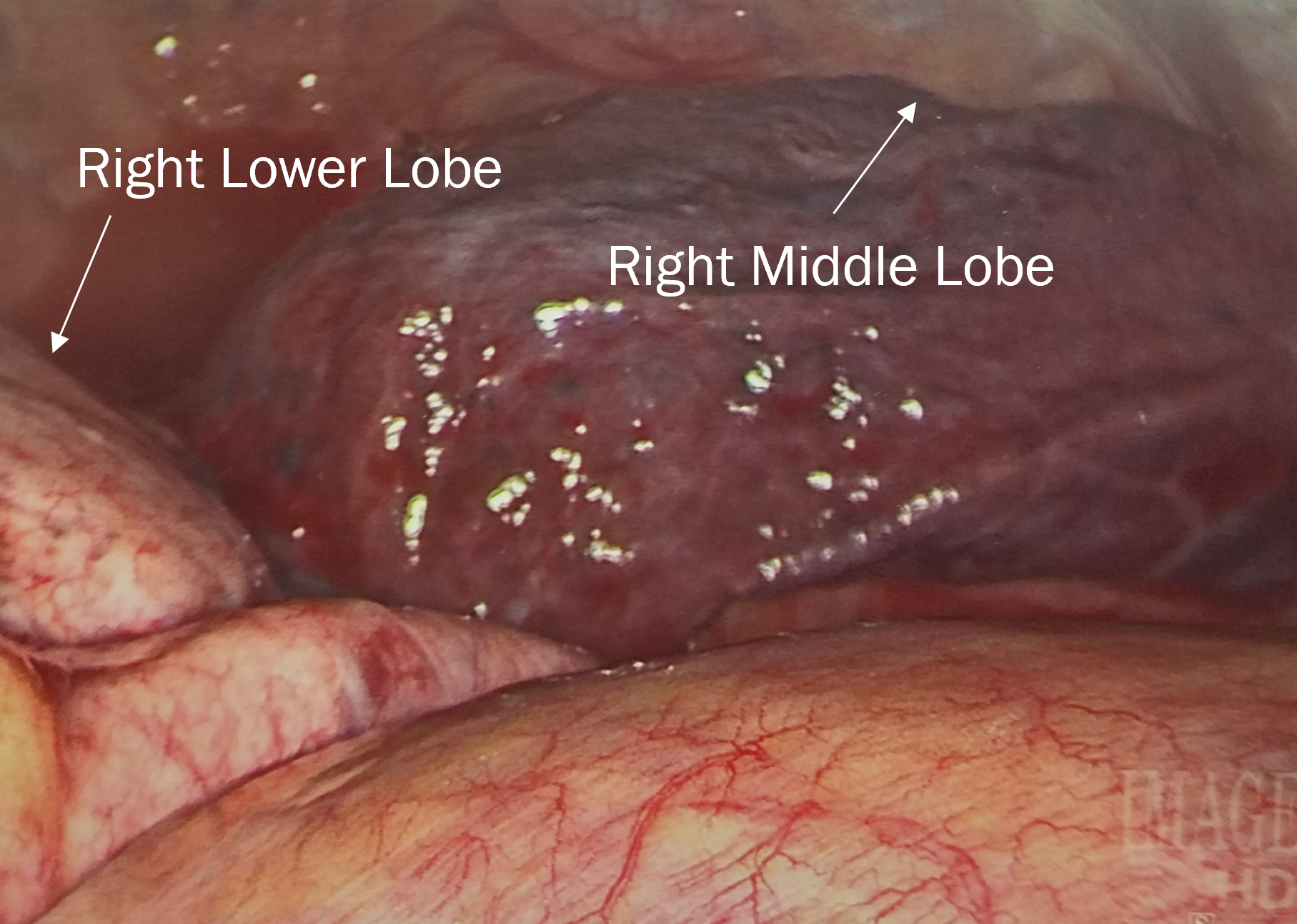
Hospital Course Part 2
- Takeback to OR:
- RML torsion
- Right VATS, Right Middle Lobectomy
- Pathology:
- RUL: Squamous cell carcinoma, pT1b pN0
- RML: Vascular congestion, focal alveolar hemorrhage
POD 1 CXR S/P Rt Middle Lobectomy
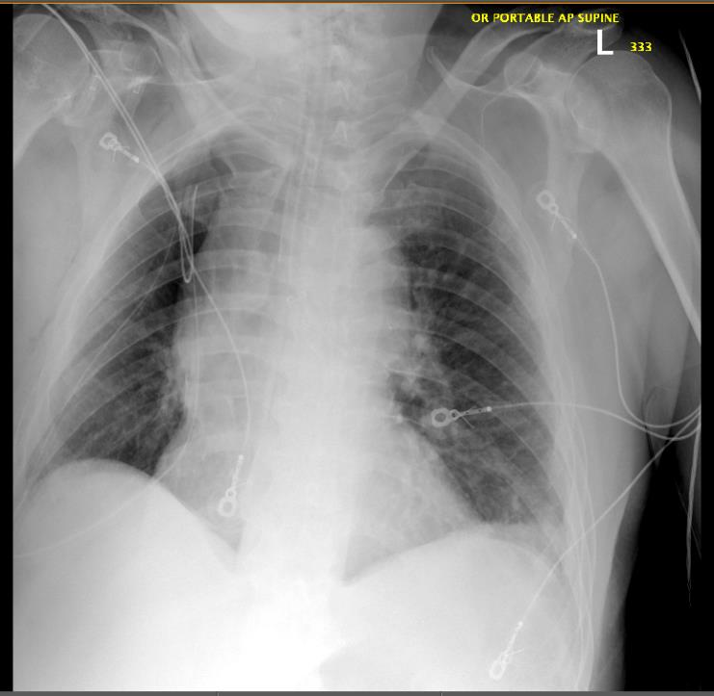
Key Points
- Differential of CXR
- Post op pneumonia
- Mucus plugging
- Right middle lobe torsion
- Differential of CT
- Shows RML collapse/consolidation
- Technical problem: 1) stapled RML airway, 2) inadvertently took RML nutrient blood supply/ischemia(right middle lobe PA +/- bronchial arteries), 3) RML torsion
- Non-Technical problem: 1) Atelectasis, 2) pneumonia, 3) RML mucus plugging
- Shows RML collapse/consolidation
- Plan
- Treat mucus plugging with bronch, pulmonary toilet. RML torsion is vascular emergency identified by airway occlusion/collapse, rare to save RML unless identified very quickly and untorsed. Best to prevent by providing broad base of attachment/fixation. If not viable on exploration, perform right middle lobectomy.
Prevention
If major fissure between middle and lower lobe is complete after an upper lobectomy:
- Close observation during reinflation of lung
- Middle Lobe Pexy - with suture, or by stapling parenchymal edge of middle lobe to lower lobe edge
- Glue has been reported in the literature (Venuta F et al. JTCVS 2012;143:240-1)