
Pet-Negative Lung Mass
Author: Alejandro Bribriesco
Institution: Cleveland VA Medical Center
Date Reviewed: December 2024
Original Case: Daniel Raymond, MD; Cleveland Clinic Foundation
Learning Domain: General Thoracic
Learning Objective: Work up of Lung Mass, Surveillance
PowerPoint File: ![]() Pet_Negative_Lung_Mass.pptx
Pet_Negative_Lung_Mass.pptx
Presentation
- 69 yo male presents with 6 months of persistent cough
- PMH: 110 pk-yr smoker; nephrolithiasis
- PSH: Inguinal hernia repair; cystoscopy with stent; lithotripsy
- Denied hemoptysis, weight loss, neuro symptoms, bone pain
- CXR reveals:
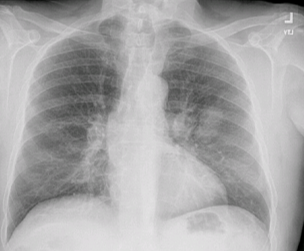
Referred to Local Oncologist
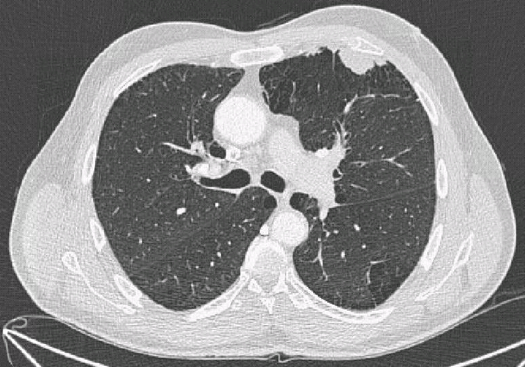
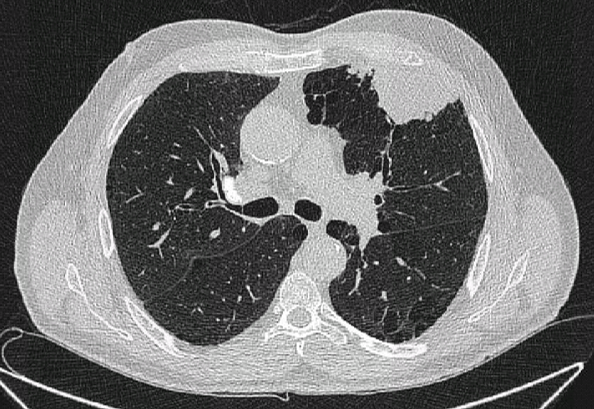
CT scan obtained: 2.7 x 1.5 cm Left Upper Lobe Mass
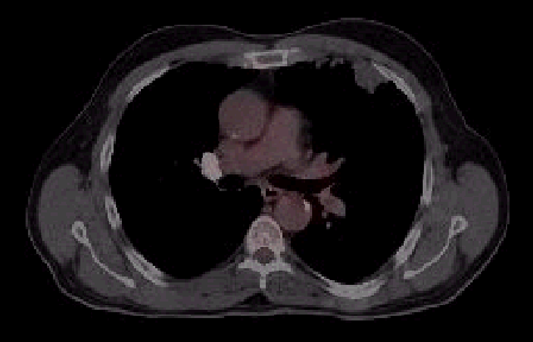
PET Scan Obtained
Report: “No FDG-uptake in lung lesion”
Core Needle Biopsy Obtained
Path report: “Small fragment of epithelial-lined inflamed fibroconnective tissue-admixed with skeletal muscle, cartilage and mucoid material . . . May represent inflammatory process, hamartoma or other unusual lesion”

Repeat CT Scan Obtained in 3 Months
Report: “Interval growth now measuring 3.7 X 1.8 cm lesion ”
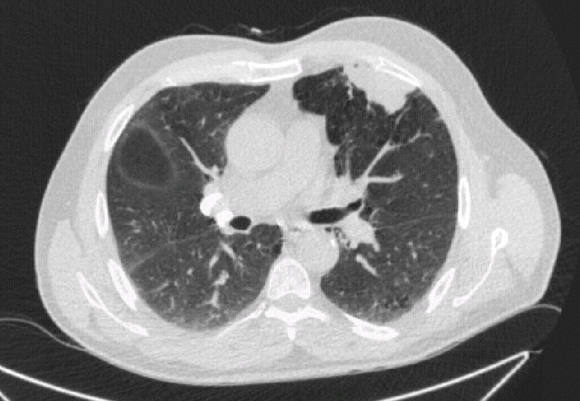
Repeat in Additional 6 Months
Report: “Continues to enlarge . . . 5.6 x 4.5 cm”
Multidisciplinary Thoracic Tumor Board
- Growing lung mass in heavy smoker high concerning for malignancy
- Based on CT scan: cT3 N0 Mx / cStage IIB
- Repeat non-surgical biopsy vs minimally invasive surgical excisional biopsy/wedge resection?
- Given high pre-test probability/suspicion: recommended proceeding with surgical resection if lymph nodes deemed negative by invasive sampling
- If occult malignancy detected: PD-L1, molecular sequencing, consideration of induction/neo-adjuvant therapy
- Staging complete
- Bronch/EBUS revealed no evidence of malignancy
- Brain MRI negative
Patient Referred to Thoracic Surgery
- Stable respiratory status, no hemoptysis, neuro symptoms or bone pain.
- Denied Chest wall pain
- Very good exercise tolerance concordant with PFTs
- FEV1 = 2.97 L (126%)
- DLCO = 20.37 (88%)
- Plan to proceed with minimally invasive exploration, left upper lobe wedge resection with intraoperative pathologic assessment
- Possible completion upper lobectomy
- Possible chest wall resection
Taken to the OR for Surgical Biopsy
- Intra-operative findings: No pleural disease, lesion not adherent to chest wall. Large wedge resection performed:
- Frozen section: Non-small cell lung cancer-adenocarcinoma
- Left minimally invasive completion upper lobectomy performed
- Final surgical path: pT2bN0M0 / pIIA mucinous adenocarcinoma
- PD-L1: 50%
- EGFR, ALK, ROS-1 negative
- Uncomplicated post-op course
- Discharged home POD#2
- Final surgical path: pT2bN0M0 / pIIA mucinous adenocarcinoma
- Subsequently referred for adjuvant systemic therapy (chemotherapy and immunotherapy)
PET (-) Malignancies
- Size, location and histologic subtype are determinants of PET avidity in lung cancer
- Low avidity histology: Bronchoalveolar cell carcinoma, well differentiated adenocarcinoma (W/D AC), mucinous adenocarcinoma and carcinoid tumors
- Size < 1 cm
- Peri-diaphragmatic location
- Due to movement
- PET NPV ~85-95%
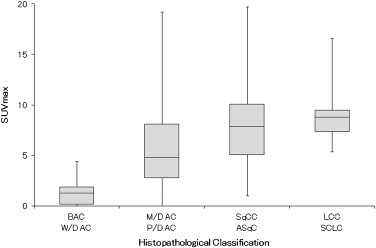
S. Iwano et al Lung Cancer 2013; 79(2): 132-6. J Wang et al Clin Lung Cancer 2012; 13(2):81-9.
False Negative Biopsy of the Lung Nodule
- Choice and accuracy of Bx modality depends on:
- Size
- Location
- Transthoracic (CT-guided) Core Needle Biopsy:
- Sensitivity: ~90% / Specificity: >95%
- Negative Predictive Value ~80%
- False negative rate: 7.48%
- Transbronchial Biopsy*:
- Sensitivity ~75% / Specificity ~60%
- Negative Predictive Value ~50%*
- False negative rate: ~20%
- *New technology (robot-assisted bronchoscopy) likely to increase accuracy
L Quint et al Cancer Imaging 2006 6(1):163-7. Schreiber et al Chest 2003 123:115S-28S. AT Ho et al Lung 2023 201(1): 85-93.
Conclusion
- A negative PET scan does not rule out malignancy
- Multidisciplinary Tumor Board is key
- Pre-text probability based on clinical context (i.e. smoking history) and tumor behavior (growth)
- Surgical biopsy may be warranted vs needle biopsy
- Mucinous adenocarcinoma of the lung
- Infrequent subtype of NSCLC-adenocarcinoma (2-10%)
- Frequently PET (-) even at large sizes given mucin deposits
- Difficult to diagnose on needle/non-surgical biopsy
- PD-L1 and molecular testing important to guide treatment strategies