
Paraesophageal Hernia
Author: Stephanie Worrell, MD
Institution: University of Arizona
Date Reviewed: 2023
Original Case: Robert B. Yates, MD; Edward Verrier, MD / University of Washington
Learning Domain: General Thoracic
Learning Objective: Benign Esophageal Disease
PowerPoint File: Paraesophageal Hernia
The Problem
- GERD is the most common foregut disease in the world and accounts for ~75% of all esophageal pathology
- Progression of the disease occurs in 13% of patients over 5 years (while on acid suppressive meds)
- Severe erosive esophagitis
- Barrett’s esophagus
- Patients at risk for progression:
- family history of GERD
- esophagitis on baseline endoscopy
- failure of esophagitis to heal with acid suppression therapy
- the need to escalate the dose of acid suppression therapy to achieve symptomatic relief
- complete dependence on daily proton pump inhibitors (PPIs) to control symptoms
Background
- Nissen has the most effective anti-reflux control
- Identification of the proper surgical candidate leads to a successful outcome in nearly all patients
- Dependent on appropriate technique
- To decrease side effects
- To decrease risk of slippage/recurrence
- Nissen associated with reliable long-term outcomes
- If concern about motility (i.e., IEM) or pre-operative dysphagia, a partial fundoplication may provide similar outcomes although some long-term data suggests inferiorly acid suppression
Identification of the proper surgical candidate
Comprehensive pre-operative work-up:
- Video esophagram
- Upper gastrointestinal endoscopy
- High resolution esophageal motility study
- Esophageal pH monitoring (off PPI in patients without Barrett's or LA Grade C/D erosive esophagitis)
Case
65yoF presents with a Type III hiatal hernia and occasional post prandial chest pain. She denies any dysphagia.
- PMH: HTN, DM, Chronic anemia
- PSH: none
- Non smoker
- PE: BP 123/84 HR 82 RR 17 O2 sat 98% RA BMI 32
- Chest CTA bilaterally, CV RRR, Abd soft NTND


Discussion Points
- Complications of PEH
- Cameron’s ulcers, volvulus (organoaxial vs mesenteroaxial), gastric outlet obstruction
- Incidence of complications if left untreated 1% per year
- Surgical Approach
- Laparoscopic vs robotic vs transthoracic
- Fundoplication
- Nissen vs Toupet vs other partial
- Adjuncts
- Collis, mesh, diaphragm relaxation, gastropexy
Operation
Robotic paraesophageal hernia repair with Toupet fundoplication:
- Given the ineffective esophageal motility on HRM and no evidence of esophagitis/BE on EGD, a partial fundoplication was chosen
- There was no evidence of a short esophagus with well >3cm of esophagus resting within the abdomen off tension following complete dissection of the paraesophageal hernia
Summary of surgical approaches
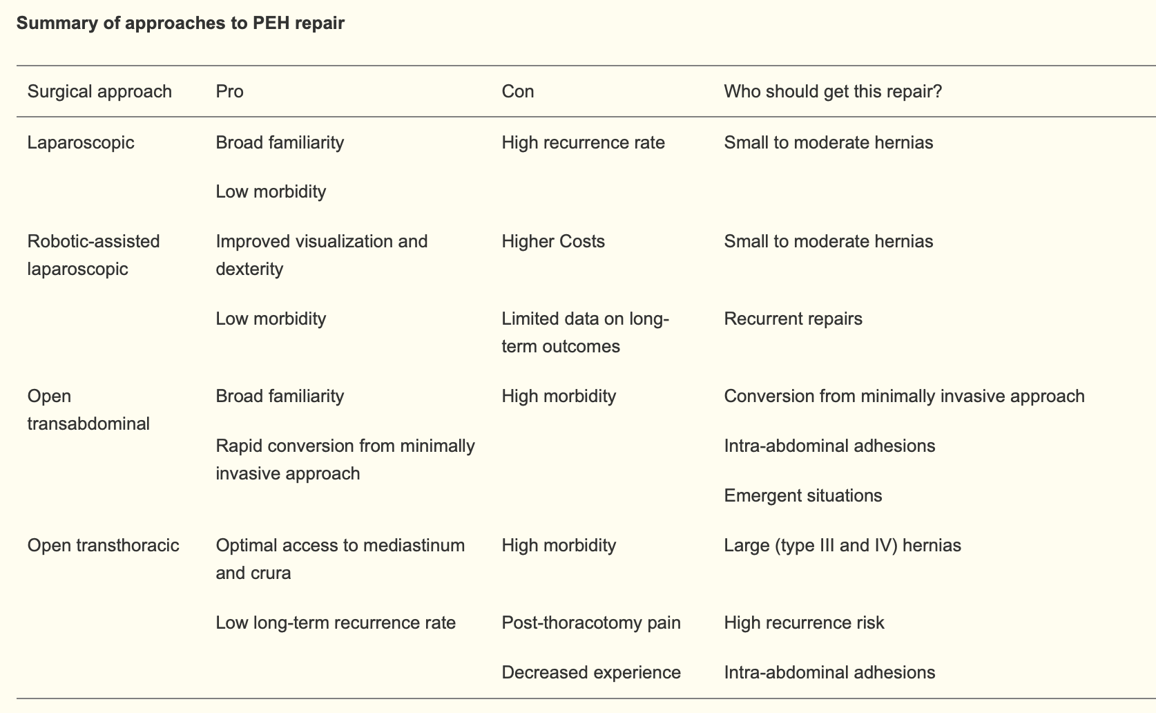
Fallon, BP & Reddy, RM (2021). Choosing the best approach for paraesophageal hiatal hernia repair: a narrative review. Video-Assisted Thoracic Surgery, 7, 7. https://doi.org/10.21037/vats-21-13
Surgical risk of PEH repair increased
- Non elective PEH repair (OR 2.06)
- Elderly, particularly >70yo (OR 1.66)
- Patients with co-morbidities
- Open approach (6.03)
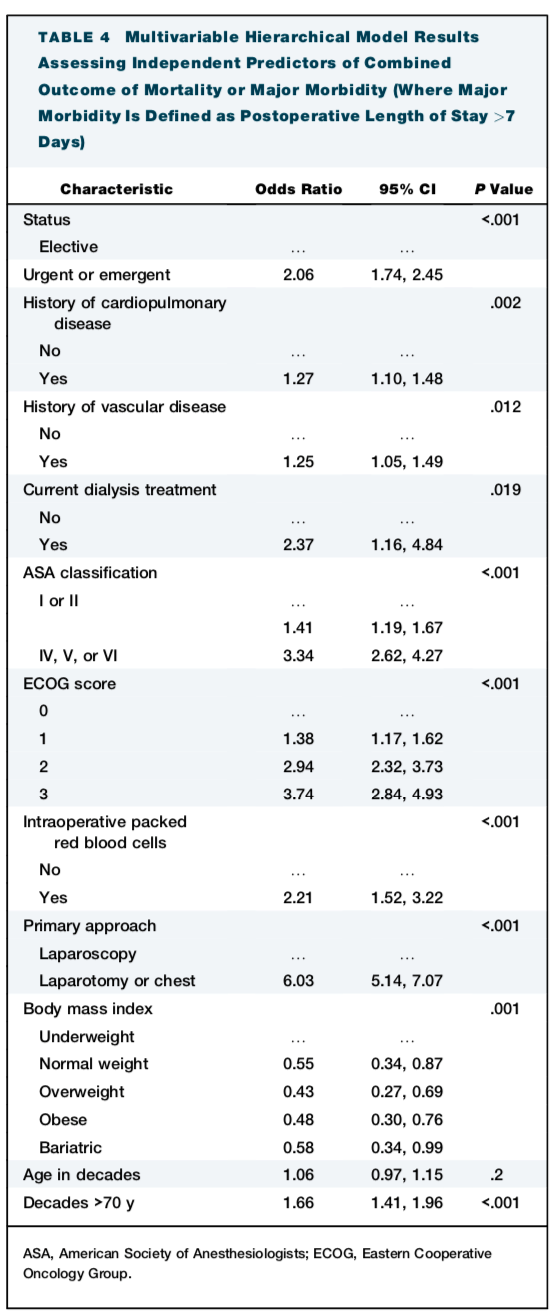
Wong, Lye-Yeng et al. The Impact of Age and Need for Emergent Surgery in Paraesophageal Hernia Repair Outcomes. The Annals of Thoracic Surgery, Volume 116, Issue 1, 138 - 145