
Iatrogenic Esophageal Perforation
Author: Stephanie Worrell, MD
Institution: University of Arizona
Date Reviewed: 2023
Original Case: David Greenhouse, MD / Massachusetts General Hospital
Learning Domain: Cardiothoracic Trauma
Learning Objective: Management of iatrogenic esophageal perforation
PowerPoint File: Iatrogenic Esophageal Perforation
Background
50-year-old male presents to the ED with chest pain. The day prior had an endoscopy done for symptoms of dysphagia. The endoscopy was significant for a mid esophageal stricture which was easily dilated to 20mm per the report. Biopsies were also don’t at the time of endoscopy and were negative for cancer.
- PMH: HTN, CAD, GERD
- PSH: none
- Meds: Aspirin, Atorvastatin, Metoprolol, Omeprazole
- Former smoker, occasional alcohol
- Physical Exam:
- HR 97 BP 165/86 RR 20 O2 sat 96% on RA
- Heart RRR, Lungs CTA bilaterally
- Abdomen soft NTND
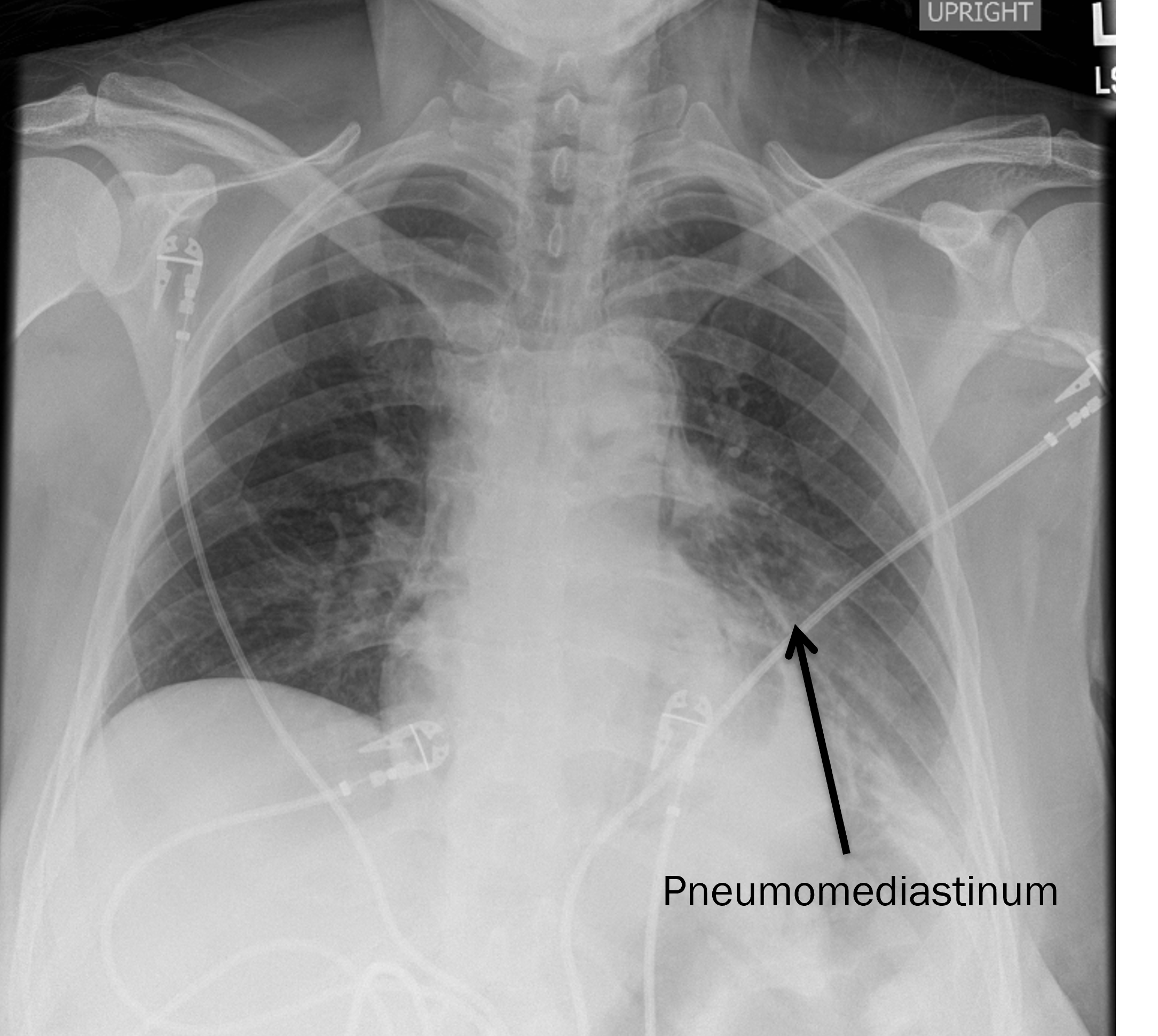
- Crepitus in the anterior chest and neck
Discussion Points
- What are the risks of iatrogenic perforation?
- How commonly does it occur?
Iatrogenic Esophageal Perforation
- Perforation rate for benign strictures: ~0.1%
- Perforation rate for achalasia dilation: 4-5%
- Risk Factors:
- A malignant stricture
- Severe esophagitis
- Prior radiation therapy
- A history of caustic ingestion
- Complex (tortuous) or long strictures
- Presence of esophageal diverticula
- Inexperienced operator
- A large hiatal hernia
- Use of high inflation pressures with balloon dilation (achalasia balloons 30-40mm)
- A history of previous esophageal perforation
- A history of prior esophageal surgery
- Prior Botox injection
Etiology of Esophageal Perforation
- More than half of esophageal perforations in adults are iatrogenic, most commonly from complex upper endoscopy
- Following iatrogenic etiology:
- Boerhave’s syndrome (15%)
- foreign body obstruction (12%)
- trauma (9%), intraoperative injury (2%)
- malignancy (1%)
- Other less common etiologies include caustic ingestion, pneumatic injury, peptic ulceration, Crohn’s disease, and eosinophilic esophagitis
Discussion Points
- What additional evaluation is indicated?
- What is the role of esophagography?
- What are the advantages/disadvantages of water-soluble contrast vs. thin barium?
- What are the advantages/disadvantages of CT?
- What are the risks and benefits of esophagoscopy?
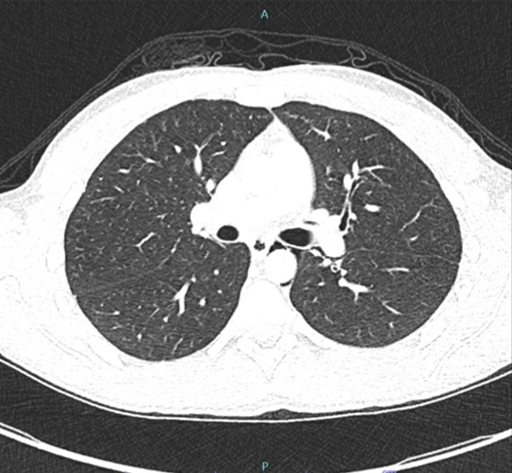
CT Scan
Management of contained esophageal perforations
- NPO/IVF
- Broad-spectrum antibiotics
- +/- enteral access
- Start diet slowly
- Liquids x2 wks
- Soft diet, slowly advance to regular
Management of uncontained esophageal perforations
- Drain the mediastinum
- VATs vs thoracotomy
- Close the hole versus divert the esophagus
- 2 layer closure with muscle flap
- Stent
- Endovac
- Feeding access
Case
- Patient made NPO and obtained esophagram
- Esophagram negative for leak
- Started on clears and sent him with oral antibiotics
Clinical Care Points
- Esophageal perforation is a rare but severe disease process that requires prompt diagnosis and treatment.
- Initial management includes resuscitation, broad spectrum antibiotics, consideration of antifungal therapy, controlling the perforation, restoring luminal integrity, and debriding all extraluminal contamination.
- Surgical intervention has historically been the mainstay of treatment, however a shift towards endoscopic treatment exists, despite no randomized clinical trials comparing patient outcomes.
- Self-expanding metal stents and endoscopic vacuum therapy have been widely described across a diverse patient population and appear to be safe and effective as a treatment strategy, in the proper clinical setting.