
Aortic Valve Insufficiency
Author: Fawwaz Shaw, M.D.
Institution: University of Washington Medical Center
Date: November 2013
Date Reviewed: March 2024
Learning Domain: Adult Cardiac Surgery
Learning Objective: Evaluation of and surgical decision making associated with acute Aortic Valve Insufficiency
History
- HPI: 33 y/o lady who presented with fever of 102.5°F, malaise and chills. She additionally reported one instance of acute blurry vision which resolved spontaneously and b/l upper arm weakness.
- PMHx: negative
- PSHX: C/Section 6 months ago.
- Social Hx: Negative tobacco, EtoH or Illicit substances. Works as a loan officer.
- Medications: None
- Family Hx: Diabetes Mellitus
Physical Exam
- Vital signs: 99/46; HR:98; Afebrile; 97% on RA
- No focal neurologic deficits.
- Normal S1, S2; Diastolic murmur. Non displaced PMI. No gallops / heaves.
- Lung fields: rales in bases, without rhonchi.
- No extremity edema
- Bilateral upper extremity weakness.
Labs
- WBC: 14.8
- Hct: 23%
- Creatinine: 1.7
- Electrolytes within normal ranges.
- Mildly elevated ALT: 72 and Alk Phos: 253.
- INR: 1.1
- Blood culture: Group B beta hemolytic Strep
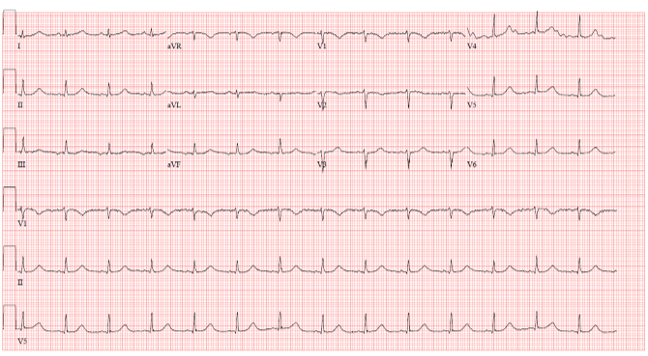
EKG
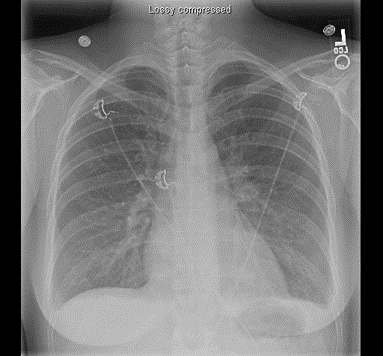
Chest X-Ray
Echocardiogram 1
Echocardiogram 2
ECHO Findings
- Severe Aortic regurgitation.
- Eccentric but broad regurgitant jet.
- Poorly visualized leaflets with probable vegetation on leaflet.
- LV size at upper limits of normal.
- Hyperdynamic function.
Additional work up?
- MRI Brain: Left parietal microinfarction.
- CT A/P: No evidence of renal, splenic or other embolic disease.
Outcome
- Underwent urgent AVR
- Pericardial reconstruction of small root abscess (1x1 cm, located on the noncoronary side of the R coronary artery).
- 19 mm Regent St. Jude mechanical prosthesis.
- Discharged post operative day #9.
- Uncomplicated post operative course.
Discussion Points
- Pre-operative work-up
- Anesthesia considerations in acute AI
- Timing / urgency of Intervention
- Pathophysiology of Acute AI
- Patient / prosthetic mismatch
- Operative management
- LV Vent / Myocardial protection / Root abscess
- Optimal Valve Choices
- Homograph / Mechanical vs Tissue valve
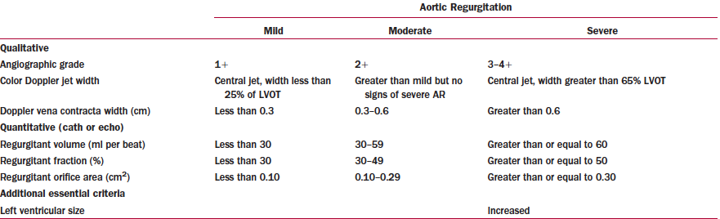
Classification of AI
Learning Points
- Acute AI differs from Chronic AI
- Treatment of acute AI is urgent surgery.
- Operation can be dependent on etiology (e.g endocarditis vs. dissection vs. trauma)
- Patients can be (acutely) very ill